 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 288-296 Review Article Pancreatic carcinogenesis: The impact of chronic pancreatitis and its clinical relevance Shrikhande SV, Barreto G, Koliopanos A Department of Gastrointestinal Surgical Oncology, Tata Memorial Hospital, Mumbai Code Number: cn09070 PMID: 19749458 Abstract Pancreatic cancer is a devastating disease with a dismal prognosis and early detection remains a challenge. On the background that inflammation is one of the key steps in the development of cancer, it is natural that chronic pancreatitis is considered as one of the etiological factors for the development of pancreatic cancer. However, the process of pancreatic carcinogenesis is a multifactorial phenomenon rather than a process that evolves solely via inflammation. This review attempts to put into perspective the association between different etiological forms of chronic pancreatitis and pancreatic cancer, and the diverse mechanisms operational in the process of pancreatic carcinogenesis. Furthermore, the clinical relevance of the current understanding of the relationship between chronic pancreatitis and pancreatic cancer, especially with regard to the pancreatic head mass of uncertain etiology, is discussed in this review.Keywords: Chronic pancreatitis, pancreatic cancer, pancreatic carcinogenesis, inflammation, pancreatic head mass, risk of pancreatic cancer Introduction Pancreatic ductal adenocarcinoma (PDAC) is the most common pancreatic malignancy and is the fourth to fifth leading cause of death in the USA, with an incidence rate of 11.2 / 100,000. [1] It is estimated that 32,180 new cases will occur in the United States in 2005. [2] In India, the incidence of pancreatic cancer is low (0.5 - 2.4 per 100,000 men and 0.2 - 1.8 per 100,000 women) in most parts of the country. [3] Despite its apparently high incidence in the West, the pathophysiology of this lethal malignancy had not been well elucidated until recently. Advances in molecular biology have greatly improved the understanding of the pathogenesis of pancreatic cancer. The molecular alterations observed include epigenetic changes such as deregulated expression of a variety of genes, gross chromosomal abnormalities, and gene mutations; all these are crucial in the development and progression of pancreatic cancer. Many patients have mutations of the K- ras proto-oncogene, and inactivation of tumor-suppressor genes. Growth factors also play an important part. However, despite the ongoing molecular research on pancreatic carcinogenesis, little progress has resulted in therapeutic benefits, and hence, the disease prognosis remains poor. Around 15 - 20% of the patients have resectable disease, but only around 20% of these survive to five years, thus reflecting the aggressive nature of the disease. [4],[5] Chronic pancreatitis (CP), is a chronic inflammatory disease of the exocrine pancreas and affects around eight patients per 100,000 population per year in the USA, with a prevalence of 26.4 cases per 100,000 population. [6] In contrast to pancreatic cancer, CP carries a much better prognosis and multiple treatment options are available to treat the main problems arising out of this disease, such as, pain and exocrine and endocrine deficiency. Ever since the first detailed description of CP by Comfort in 1946, [7] many different forms of CP have been described. It is now known that mutations in the cationic trypsinogen gene are present in patients with hereditary CP, and it has been reported that approximately 30% of the patients with so-called idiopathic CP have mutations in the cystic fibrosis transmembrane conductance regulator gene. [8],[9],[10],[11] Although the morphological changes in CP have been recognized and described for many decades, the pathophysiology of CP is still poorly understood, and it is not known whether the pathophysiological events in different CP etiologies are similar or diverse. In the Western industrialized countries, the dominant etiological factor of CP is alcohol abuse, accounting for approximately 80% of patients. [12] In a small percentage of patients with CP, alcohol abuse can be clearly ruled out as an etiological factor, and if other known etiological factors are absent, these patients are then classified as having idiopathic CP. [12],[13] In contrast with Western countries, in India, especially southern India, an alcohol independent form of CP - tropical pancreatitis - is common. [12] Here there is a chronic calcifying form of CP, in a younger age group, in a region of high incidence, without any history of alcohol consumption. The etiology of tropical CP is largely unknown, and nutritional and environmental factors have been propagated since the 1970s and 1980s, as being the major causative factors in the etiopathogenesis of this form of CP. [14],[15] More recently, SPINK 1 mutations have been implicated as the causative factors of tropical CP. [16],[17] Irrespective of the underlying etiology, CP is characterized by a continuum of progressive parenchymal destruction, ductal strictures, atrophy of acinar and islet tissue, de-differentiation of acinar cells into tubular complexes, immune cell infiltration and inflammation, alteration of nerves, and progressive fibrosis. [18] Chronic inflammation, the dominant morphological feature of CP, is known to cause neoplastic transformation and it is not surprising that chronic pancreatitis (CP) is considered to be associated with an increased risk of pancreatic cancer. The recognition of the entity of autoimmune pancreatitis has further complicated the picture. The main issues are:
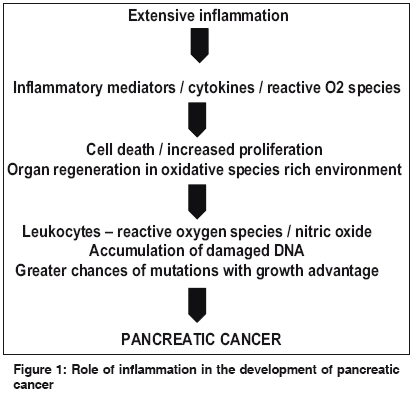
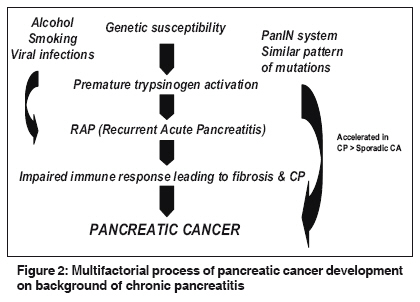
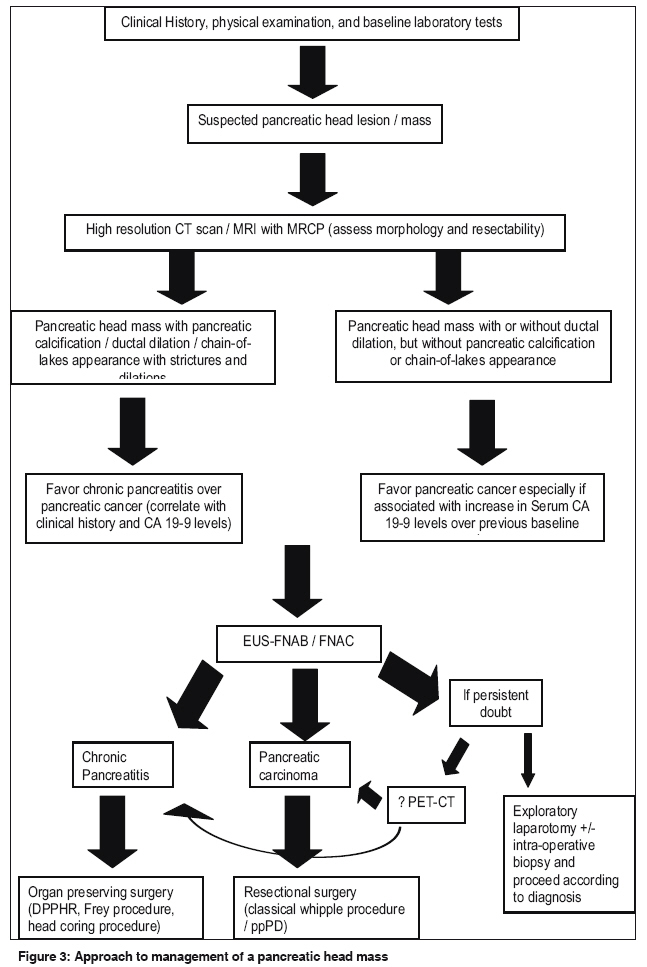
Risk of Pancreatic Cancer in CP: Epidemiological, Experimental, and Clinical Data Alcoholic CP The risk of development of cancer in alcoholic CP increases with increasing duration of the disease. In the landmark study by Lowenfels et al ., [19] it was observed that the risk was 1.8 and 4% at 10 and 20 years of alcoholic CP. The difficulty in evaluating the pathway of progression of Alcoholic CP into pancreatic cancer is complicated by the incidence of other life-threatening sequelae (Cirrhosis / Portal hypertension) that may intervene at an earlier stage, often long before CP causes oncogenic transformation in the affected pancreas. Tropical and cystic fibrosis associated CP Considering that the disease is characterized by an early age of onset (as compared to alcoholic CP), the changes induced by prolonged inflammation can therefore be better evaluated. In an observational study by Ramesh et al ., it was noted that 22 out of 266 patients with tropical CP developed pancreatic cancer, with a high risk of cancer in tropical CP of 8.3%. [20,21] Chari et al ., reported that over a 4.5-year period, 24 of 185 patients with TP died and that six (25%) died of pancreatic cancer. The average age of onset was 45 ± 7 years, and the relative risk of pancreatic cancer compared to those without TP was 100 times normal. [22] Similar rates have been noted with cystic fibrosis associated CP. [23],[24] Hereditary CP In the Europac study, the largest ever study evaluating the role of hereditary CP in development of pancreatic cancer, 418 patients from 112 families in 14 countries were evaluated and it was noted that the cumulative risk of pancreatic cancer was 8.5% at 40 years, in this form of CP. [25] A follow-up report from the original international study by Lowenfels [26] included 497 patients with hereditary pancreatitis, with 19 cases of pancreatic cancer compared with an expected number of 0.33, yielding a risk ratio of 57 (95%CI : 35 - 90). Both these studies, thus confirm, a high risk of pancreatic cancer in patients with hereditary pancreatitis, irrespective of the underlying mutation. The above data based predominantly on epidemiological studies, indicates an increased likelihood of the development of pancreatic cancer in patients who have CP. Role of CP in Oncogenic Transformation: Experimental Data Extensive and prolonged inflammation results in the release of inflammatory mediators, cytokines, O 2 radicals, and upregulated inflammatory pathways. These events lead to cell death with increased proliferation, with organ regeneration in an oxidative-species-rich environment. These events create a situation where damaged DNA accumulates and this ultimately leads to pancreatic cancer. [27],[28] [Figure - 1] shows the process of oncogenic transformation on the background of inflammation. Although this hypothesis seems attractive, it must be borne in mind that only 10% of chronic inflammatory conditions ultimately progress to cancer, [29] for example, chronic obstructive pulmonary disease resulting in lung cancer. Also, while it has been proposed that the findings in different etiological forms of CP are essentially similar and a common "surgical stage of CP" is reached despite the different pathways they initially follow, [30] the incidence of development of cancer is not uniform in these different forms of CP, as discussed in the preceding sections. It is thus apparent that other factors, in addition to inflammation, are operational in CP leading to development of pancreatic cancer. Process of Oncogenic Transformation is Multifactorial In addition to inflammation in CP, it appears that genetic susceptibility (causes premature trypsinogen activation with development of recurrent acute pancreatitis (RAP)), alcohol abuse, smoking, and viral infections also promote pancreatic parenchymal injury in susceptible individuals and cause RAP. In a multivariate analysis of 497 patients with hereditary CP, Lowenfels [26] has found that smoking independently doubled the risk of pancreatic cancer, which even developed 20 years earlier in smokers compared to nonsmokers and accounted for approximately 25 - 30% of all pancreatic tumors. RAP leads to inflammation, fibrosis, and CP, which ultimately results in cancer. The PanIN system (noninvasive precursors of invasive pancreatic ductal adenocarcinoma) is a series of pathologic changes that correspond with various genetic alterations, which ultimately lead to the stage of preinvasive cancer. [31] Although, Pancreatic Intraepithelial Neoplasia (PanIN), [32] which refers to a microscopic papillary or flat-invasive, epithelial neoplasm arising in the pancreatic ducts (< 5mm) and is characterized by columnar-cuboidal cells with varying amounts of mucin and degrees of cytologic and architectural atypia, was earlier believed to occur only in pancreatic cancer, there are reports that PanINs can develop without cancer. One such condition in which they do occur is CP. [32] PanINs appear to run an accelerated course in CP compared to sporadic pancreatic cancer. [Figure - 2] shows the multifactorial process of pancreatic cancer development on the background of CP. Molecular Markers for Differentiating CP from Pancreatic Cancer Genetic studies of oncogene mutations are useful in expanding our knowledge on the relationship between CP and pancreatic adenocarcinoma. In a prospective study of 76 patients with CP (59 alcoholic, 15 idiopathic, and 2 hereditary), van Laethem [33] examined K-ras mutations in collected ductal brushings during therapeutic ERCP, and after a long-term follow-up, every 6 - 12 months, K-ras (codon 12) mutations - GAT and GTT in a majority of the cases - were found in 25% of the patients, quite similar to those found in adenocarcinoma. There was no relationship between the presence of mutant K-ras and the etiology of CP (alcoholic: 20% of mutant K-ras; idiopathic: 30%; hereditary: 50%), the duration of the disease before the analysis, the presence of acute attacks, the existence of pancreas divisum, or the presence of a pancreatic stent. p53, p16, and Smad 4 mutations have also been evaluated as markers differentiating CP from pancreatic cancer. In fact, Talar-Wojnarowska et al . [34] in a review of the available literature on the incidence of specific sequences of oncogenes and tumor suppressor genes, including K-ras, Her-2/neu, p16, p53, and DPC4, found that the incidence of mutations of K-ras, p16, and p53 were much more common in pancreatic cancer as compared to CP. However, the current findings are not specific and sensitive enough for their routine clinical recommendation. [35] DPC4 staining of ducts seen in CP is lost in about half of the patients with pancreatic cancer. [36] On the other hand, Ki-67, a marker of proliferative activity of neoplastic cells is much higher in pancreatic cancer as compared to CP. [36] Another immunohistological marker that may be useful in differentiating the two entities, is MUC1, which is not expressed in CP, but may be found in pancreatic cancer. [36] New evidence is emerging on the role of micro RNAs (miRNA) in differentiating CP from pancreatic cancer. Bloomston et al . [37] found 15 overexpressed and eight underexpressed miRNAs in cancer. These included miRNA 221, a hitherto unreported miRNA in pancreatic cancer that has been found in thyroid cancer and is associated with angiogenesis. [37]. Based on proteomic analysis of tissue specimens from pancreatic cancer and CP, it has been found that expression analysis of UHRF1, ATP7A, and aldehyde oxidase 1, in combination, could potentially provide a useful additional diagnostic tool for fine-needle aspirated or cytological specimens obtained during endoscopic investigations. [38] Pancreatic Head Mass: Chronic Pancreatitis or Cancer? Complications of CP may affect the gland or the surrounding structures. Among others, CP can result in the development of an inflammatory head mass, which can become a considerable source of diagnostic confusion. It has been reported that an inflammatory mass larger than 4 cm may occur in as many as 75% of the patients requiring surgery for CP. [39] Such an inflammatory mass often raises suspicions of pancreatic cancer in the mind of a treating surgeon. Clinical Features Overlap in imaging studies, clinical findings, and treatment options frequently leads to confusion in diagnosis and management. [40] Differentiating between CP and pancreatic cancer can therefore prove to be extremely difficult due to this overlap in the signs and symptoms of each disease. Epigastric pain, weight loss, steatorrhoea,-associated diabetes, and obstructive jaundice are observed in both cancer and inflammation; however, they may occur in varying frequencies. [40] While CP usually has the classical picture of longstanding epigastric pain radiating to the back, history of alcohol consumption in the western countries, previous acute exacerbations, and history of chronic analgesic intake, the disease may often appear without an apparent previous history [41] and raise the doubt of pancreatic cancer in the clinicians mind. On the other hand, painless progressive jaundice, classical of a malignant lesion, is uncommonly associated with CP. However, a high index of suspicion and attention to clinical detail may aid in reaching a precise diagnosis. Malignant transformation should be suspected when "new symptoms" develop in an established longstanding case of CP, such as, sudden and severe weight loss in a controlled diabetic or the development of jaundice. Despite a high index of suspicion, pancreatic cancer is missed in 2 - 4% of patients undergoing pancreatic duct drainage for presumed CP. [42] Conversely, many series have reported a 5 - 10% inadvertent resection rate for "pancreatic cancer" ultimately proved to be CP. [43],[44],[45] It is thus clear that additional inputs are necessary in some patients to arrive at a diagnosis, even after a detailed history and the best of clinical examinations. Laboratory Investigations CA 19-9 This tumor marker was first described in 1982 by Koprowski and his associates. [46] It is the most widely used conventional marker for pancreatic cancer and is a useful tool in the diagnosis and follow-up of patients after resection. However, its role in the early detection of pancreatic cancer is limited. The sensitivity of CA 19-9 is > 80% in pancreatic cancer, but the specificity is lower. [47] It has been suggested that a subsequent rise of CA 19-9 after postoperative normalization may precede clinical detection of recurrent disease. [48] Elevation of CA 19-9 levels corresponds to advanced disease and poorer outcomes in pancreatic cancer and even in gastric cancer. In a study evaluating the expression of CA 19-9 in normal pancreas, chronic pancreatitis, and pancreatic cancer, elevated levels were observed in 87% of the patients with pancreatic carcinoma compared to only 13% in the group of benign disease. [49],[50] Currently, an elevation of serum CA 19-9 over previous baseline levels should be viewed with suspicion from the point of view of a malignant transformation. To date, there is no other specific laboratory investigation that might aid in differentiating pancreatic cancer from an inflammatory mass of CP. Imaging CT scan The sensitivity of a CT scan is around 83% and the specificity 93% for ductal carcinomas [51] . In CP, the imaging features are ductal dilation, parenchymal calcification, and a chain-of-lakes appearance (mainly in tropical CP), often with ductal calculi, in addition to enlargement of the pancreatic head. Furthermore, as the disease progresses, the gland may look small and atrophic due to the ongoing fibrosis. On the other hand, pancreatic head cancer shows a slightly hypovascular lesion with irregular borders. [52],[53] Also, pancreatic calcification is uncommon. However, as seen in CP, pancreatic duct obstruction also occurs in pancreatic cancer with resultant ductal dilatation, and this can lead to a diagnostic dilemma. Magnetic resonance imaging (MRI) MRI with cholangiopancreatography (MRCP) has now been accepted as a technique that is able to completely replace diagnostic ERCP. When initially described in the mid 1990s, further studies were necessary for a better evaluation of the potential advantages and disadvantages of this technique. [54] The advantage of this technique is that the bilio- pancreatic ductal anatomy is better delineated, without any contrast injection being required. Although by no means 100% accurate, ultrafast MRI (UMRI) is now reported to be equal or even superior to all other staging methods. It has replaced other methods in many centers, because it provides an "all-in-one" investigation, avoiding endoscopy, vascular cannulation for angiography, allergic reactions, and radiation. However, it is not yet perfect and hence the final verdict on resectability of a pancreatic head mass still depends on surgical exploration in some cases. [55] Positron emission tomography (PET) (18)F-FDG PET scan imaging has been shown to be a useful tool in the diagnosis of pancreatic cancer and even to detect metastasis in patients post chemoradiotherapy. [56] It is also known to be useful in differentiating benign from malignant lesions based on an increased standardized uptake value (SUV) measured at two different time points. [57] An early experience with this technique in differentiating pancreatic cancer from chronic pancreatitis was demonstrated by Lan et al . [57] Thereafter, Bang et al . [58] have provided evidence to support the role of PET-CT as being an effective modality in detecting pancreatic cancer. However, further studies comparing the ability of PET imaging to differentiate cancer from pancreatitis are awaited before its place in the diagnostic Figure of an undifferentiated mass of pancreas can be confirmed. Endoscopic Ultrasonography (EUS) EUS has gained much attention, as it eliminates the problems of gas and obesity seen with the conventional ultrasound and can detect small pathologies, especially in the periampullary region, in experienced hands. EUS-guided fine needle aspiration of the pancreas (FNA) has a sensitivity of 80% and specificity of 82% in detecting tumors, [59] and this is an attractive concept in situations where a pathological diagnosis is necessary prior to initiating some form of treatment. [60] Horwhat et al . [60] in the randomized cross-over trial comparing EUS-guided FNA to CT-guided FNA were able to demonstrate a high sensitivity of 84% for EUS, as opposed to 62% for CT-guided FNA. Their study, however, was underpowered, leading to a non-significant p value. Although, what the study did confirm was that no malignancies were missed in the EUS-guided FNA group. However, the sensitivity of the EUS-guided FNA falls to around 54% when used for diagnosing pancreatic cancer in chronic pancreatitis. [61],[62] Thus, while EUS is highly sensitive in detecting abnormal masses in cases of CP, the positive predictive value of the diagnosis of pancreatic cancer is low. [63] The reasons ascribed to this are the difficulty in targeting the exact lesion, coupled with the presence of fibrosis and inflammation in the surrounding pancreas. [64] A recent work by Moller et al . [65] seems to indicate that combining the histological examination of core biopsies with cytological analysis (both obtained by EUS-guidance), can actually result in a higher sensitivity, with a lower number of biopsies required. Do Combinations of Tests Improve Diagnostic Yield? It has been reported [48] that a combination of CA 19-9 and ultrasound improved the sensitivity of each test by 10 - 15%. Currently, a careful, detailed history and clinical examination along with a high resolution contrast-enhanced CT scan and serum CA 19-9 levels would seem to be the best combination available to reach a likely preoperative diagnosis in a pancreatic head mass of uncertain etiology. Intra-operative Diagnosis In many instances, surgeons rely on an exploration in the case of pancreatic head masses of uncertain etiology, when the clinical picture and investigations do not exclude a malignancy. In these cases, trying to reach an intra-operative diagnosis may be complicated by findings that are equivocal for an ampullary or pancreatic head lesion or CP, such as, obstruction of the main pancreatic duct, a surrounding desmoplastic reaction, and so on. However, the main pancreatic ductal dilation with multiple strictures, calculi, pseudocysts, and parenchymal calcification are some of the features that would favor a diagnosis of chronic pancreatitis in a head mass rather than pancreatic cancer. While a fine needle aspiration (usually a transduodenal route) in combination with an intra-operative ultrasound may help reach a diagnosis, [66],[67] the surgeon may often have to resort to a pancreaticoduodenectomy. In the variant of autoimmune pancreatitis (which responds best to steroid treatment), the whole gland is usually affected and a distinctive head mass can often not be appreciated. [68] Approach to Treatment Whenever there is a possibility of cancer, pancreatic resection should be performed, as it is both diagnostic and therapeutic. In a study evaluating "blind" Whipple resections for periampullary and pancreatic lesions, without a prior diagnosis of malignancy, clinical judgment was observed to be correct in 90% of these patients. [69] This study reported that in patients with potentially resectable lesions (based on CT scan examination), biopsy information did not affect the choice of therapy, since a negative biopsy still committed the patient to surgery and the study was concluded by questioning the practice of numerous biopsy attempts in patients with periampullary lesions. [Figure - 3] provides a broad outline for management of a pancreatic head mass. Summary There is increasing evidence that pancreatic carcinogenesis is a multi-step phenomenon. Molecular diagnostic methods such as detection of K-ras mutations in pure pancreatic or duodenal juice, in addition to fine needle aspirations, can achieve earlier diagnosis of pancreatic cancer in selected subgroups, for example, in patients with CP. [70] Redirection of experimental work toward pancreatic inflammation and mechanisms of carcinogenesis may identify other novel anti-inflammatory agents or other methods to screen and even prevent pancreatic cancer. Potential markers (e.g., Annexin A4, Cyclophilin A, Cathepsin D, S100A8, etc.), unique to pancreatic cancer compared to the normal pancreas and CP, have recently been identified by using a proteomic approach of two-dimensional (2D) gel electrophoresis and mass spectrometry. They may eventually serve as diagnostic markers or therapeutic targets [71] in pancreatic tumors. miRNAs have also been described, which may help in differentiating the two entities. With regard to the treatment where a dilemma exists between pancreatitis and cancer, the most important variable would be the surgeon himself and his team. The more experienced the pancreatic surgeon, the more likely it is for a major pancreatic resection to be performed with minimal morbidity and mortality, and an aggressive approach can be pursued in experienced centers so that some cancers get curative resection, and if the diagnosis ultimately turns out to be CP, an adequate relief from symptoms is maximally achieved. As far as autoimmune pancreatitis is concerned, a high index of suspicion needs to be maintained, to improve the rates of diagnosis, and unnecessary surgery has to be avoided. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09070f2.jpg] [cn09070f1.jpg] [cn09070f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}