 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 311-317 Original Article Cisplatin-based chemotherapy: Add high-frequency audiometry in the regimen Arora R, Thakur JS, Azad RK, Mohindroo NK, Sharma DR, Seam RK Departments of Otorhinolaryngology-Head and Neck Surgery, I G Medical College, Shimla Code Number: cn09073 PMID: 19749461 Abstract Background : Cisplatin-induced ototoxicity shows high interindividual variability and is often accompanied by transient or permanent tinnitus. It is not possible to identify the susceptible individuals before commencement of the treatment. We conducted a prospective, randomized and observational study in a tertiary care centre and evaluated the effects of different doses of cisplatin on hearing.Materials and Methods : Fifty-seven patients scheduled for cisplatin-based chemotherapy were included in the study. All patients were divided into three groups depending on the dose of cisplatin infused in 3 weeks. Results : The subjective hearing loss was found in seven patients, while six patients had tinnitus during the chemotherapy. The hearing loss was sensorineural, dose dependent, symmetrical, bilateral and irreversible. Higher frequencies were first to be affected in cisplatin chemotherapy. Conclusion : As use of high-frequency audiometry is still limited in research work only, we need a strict protocol of adding high-frequency audiometry in the cisplatin-based chemotherapy regimen. Keywords: Audiometry, cisplatin, hearing loss Introduction Cisplatin contributed significantly in the early success of modern chemotherapy for solid tumors and today, cisplatin is a primary drug for testicular cancer, medulloblastoma, osteogenic sarcoma, cervix and ovarian cancers. Cisplatin is a cell cycle-nonspecific cytotoxic drug and has a toxic profile that is different from other important cytotoxic drugs. High doses of cisplatin cause nephrotoxicity, gastrointestinal toxicity, neurotoxicity and ototoxicity. Ototoxicity is one of the dose-limiting side effects of cisplatin because it increases with increase in the dose. [1],[2] Initially, [2],[3] it normally manifests as high-frequency sensorineural hearing loss that may progress to affect frequencies within the speech range later in the treatment. Cisplatin-induced ototoxicity is often accompanied by transient or permanent tinnitus [4],[5] and shows high interindividual variability. [6] Exact etiopathogenesis of this high intraindividual variability is still unknown but pharmacokinetic differences, genetic factors and metabolic status of the individuals are implicated. Identification of susceptible individuals before commencement of the treatment is not possible; however, early ototoxic effects can be detected by high-frequency audiometry [7] and otoacoustic emission. [8],[9],[10] We conducted a prospective, randomized and observational study and evaluated the effects of different doses of cisplatin on hearing. Materials and Methods This study was conducted in the Departments of Otolaryngology- Head and Neck Surgery, and Radiation-Oncology (Regional Cancer Centre). Fifty-seven patients scheduled for cisplatin-based chemotherapy were included in the study. We divided all the subjects into three groups:
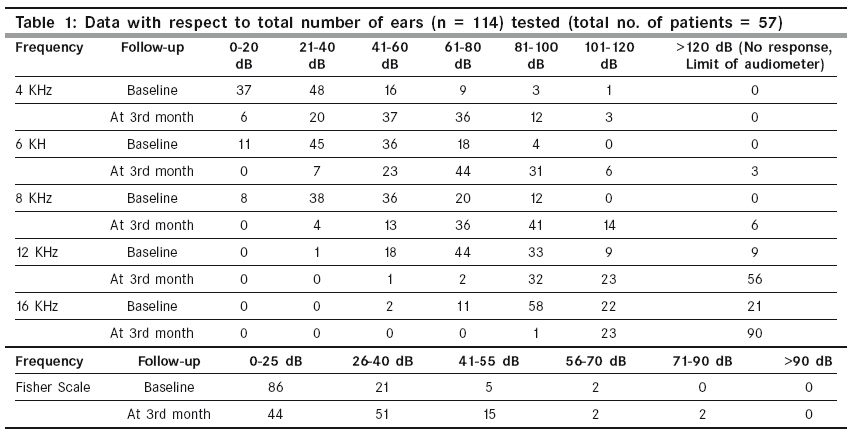
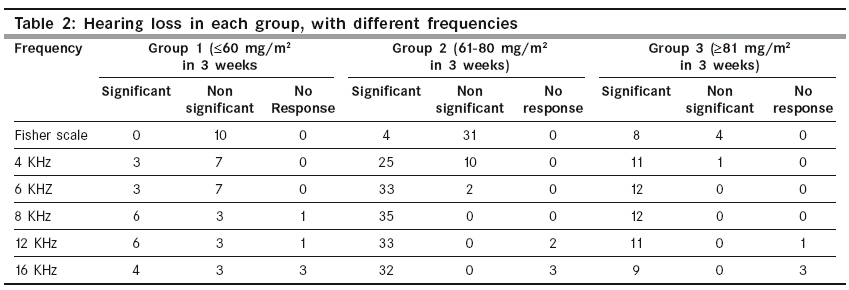
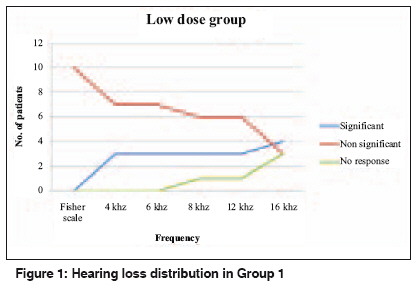
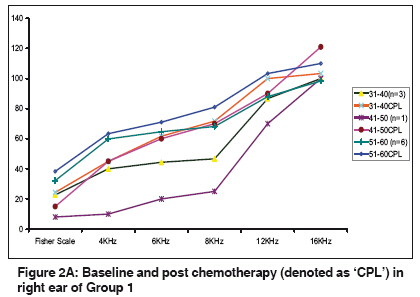
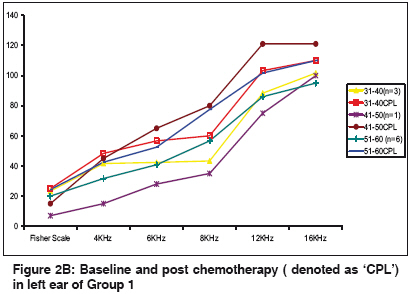
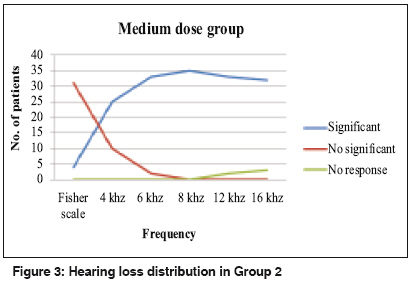
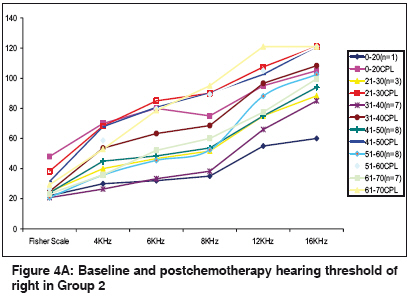
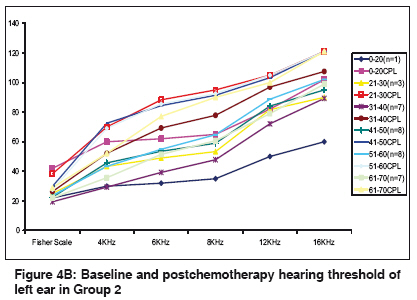
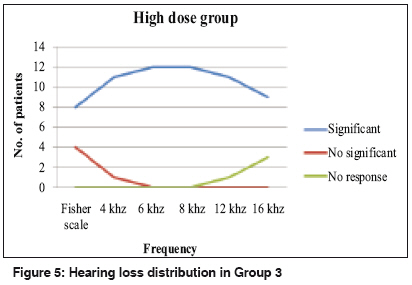
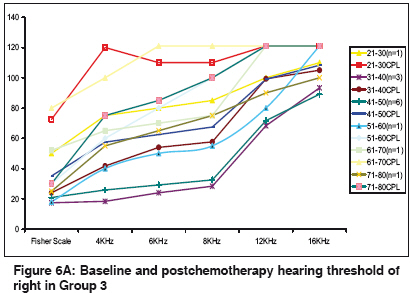
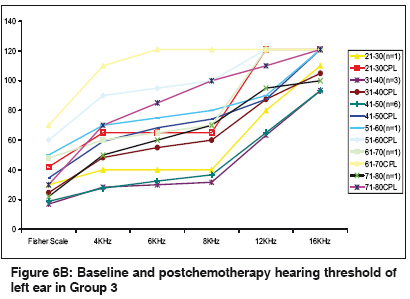
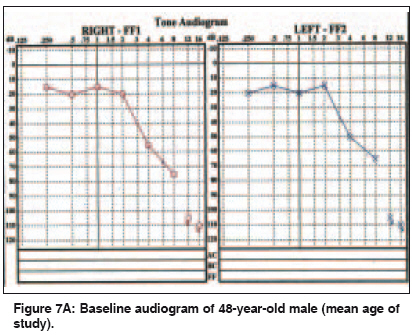
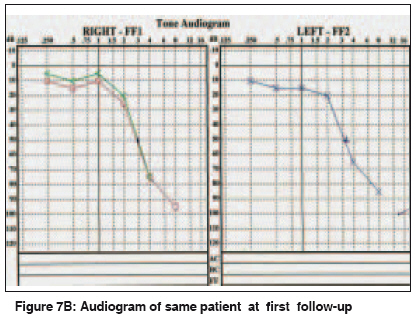
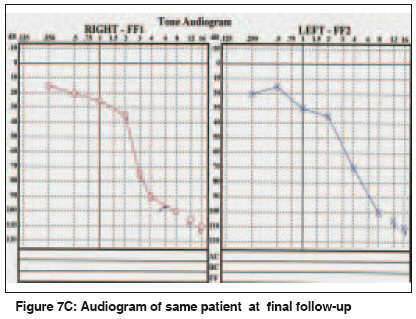
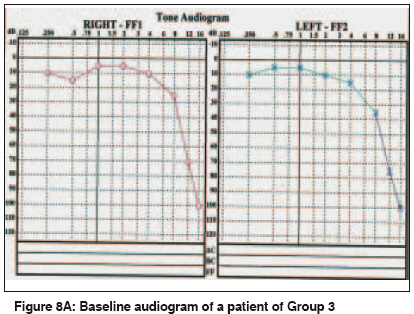
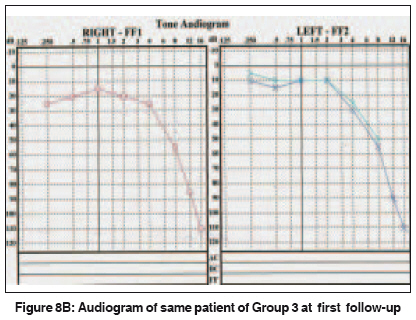
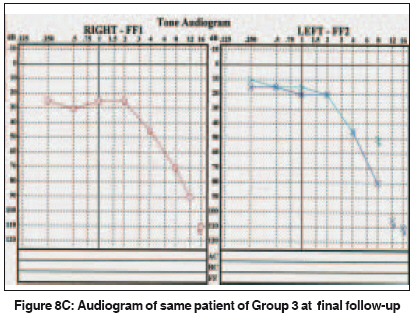
Prior to the start of chemotherapy, a baseline hearing threshold data (up to 16 KHz) was obtained by a pure-tone audiometer (Clinical audiometer AC 40, manufactured by Interacoustics A/S, DK-510, Assens, Denmark) installed in a sound-proof room of the otolaryngology department. Patients were reassessed after 1 and 3 months of last cisplatin infusion. The frequency spectrum of hearing loss (HL) was recorded in each subject. Statistical package SPSS 13.0 was used to evaluate the probability of significance. Postchemotherapy, a increase of 10 dB at Fisher′s scale (mean value of hearing thresholds at speech frequencies, i.e., 0.5, 1 and 2 KHz) and increase of 20 dB at individual frequency from the baseline hearing threshold was considered significant ( P < 0.05 was observed at 95% CI using chi-square test). During baseline audiometry, a frequency with absent response (hearing threshold> 120 dB) was excluded from the observations. On follow-up, if a subject with previous response at a frequency develops an absent response on that frequency then this was significant, and a value of 121 dB was taken for chart preparation. Results In this study, patient age ranged from 19 to 76 years, with the majority of patients aged 40-50 years. The mean age of presentation was 48 years. The male to female ratio was 1.8:1. In 57 subjects (114 ears), mean baseline hearing threshold at all tested frequencies was 54.4 dB, which increased to 73.1 dB after 3 months [Table - 1]. During follow-up, seven patients complained of subjective hearing loss and six had tinnitus at the time of first follow-up but none had both complaints. The tinnitus was present in one subject of Group 1 (50-year-old male) and group 3 (34-year-old male), while group 2 had 4 patients (mean age 50 years). There was no statistical correlation between age and dose of cisplatin. There was no subjective or objective vertigo in any patient. Group 1 [Table - 1],[Table - 2] and [Figure - 1] had mean age of 45.82 years and all 10 subjects received cisplatin at 50 mg/m 2 . All subjects had insignificant changes at Fisher′s scale. Of 10 patients, 3 had significant hearing loss at 4 and 6 KHz. Of 9 patients, 6 had significant hearing loss at 8 and 12 KHz, while only 4 of 7 patients showed significant hearing loss at 16 KHz. The maximum increase in the hearing threshold after cisplatin was 45 dB at 8 KHz in both ears in the 41-50 year age group, which had only 1 patient [Figure - 2A and 2B] . Group 2 [Table - 1],[Table - 2] and [Figure - 3] had a mean age of 49.47 years and all patients received cisplatin at 80 mg/m 2 . In this group, 4 patients had significant hearing in the Fisher′s scale. Hearing loss observed in all patients was > 8 KHz. In this group, cisplatin caused the maximum increase of 40 dB at 12 KHz in the hearing threshold of right ear in a 19-year-old patient [Figure - 4A]. In the left ear, uniform increase of about 30 dB was observed in hearing threshold at all frequencies in all age groups [Figure - 4B]. Group 3 [Table - 1],[Table - 2]; [Figure - 5] had a mean age of 45.16 years. Eight patients had significant hearing loss at Fisher′s scale and this loss was observed in 11 of 12 patients at 4 and 6 KHz. All subjects in this group had hearing loss at 8, 12 and 16 KHz. The maximum increase in hearing threshold was> 60 dB at 6 KHz in both ears of a 63-year-old patient [Figure - 6A and 6B]. [Figure - 7A-7B-7C] shows baseline, first and final audiograms of a 48-year-old patient (mean age of study) while [Figure - 8A-8B-8C)] shows similar audiogram of a patient belonging to Group 3. In all three groups, hearing loss was sensorineural, irreversible and symmetrical, and there was no sex predilection. Discussion Cisplatin induced ototoxicity compromises, [11] development of language, cognitive functions, learning ability, communication and quality of life in terms of isolation and depression. The exact cause of cisplatin toxicity is still unclear. [12] The unbound cisplatin in the plasma is responsible for its toxicity. Cisplatin blocks transduction channels within the outer hair cells of the cochlea and causes progressive destruction of outer hair cells, inner hair cells and supporting cells within the organ of Corti. Hair cell loss in the vestibular labyrinth and injury to the stria vascularis also occurs. Cisplatin ototoxicity is also associated with the generation of reactive oxygen species, depletion of intracellular glutathione and interference with antioxidant enzymes within the cochlea. In this study, hearing assessment was done before starting cisplatin therapy and at one and three months after cisplatin infusion. In majority of the patients, hearing loss was found at the time of first follow-up, i.e., one month after cisplatin administration. This hearing loss was progressive and irreversible on second follow-up, i.e., three months after cisplatin infusion. Berg et al. [13] conducted a study of cisplatin in children and also observed hearing losses in children as early as one month. Few studies [14],[15] involving follow-up to two years had also found irreversible hearing loss by cisplatin. We found no correlation between age and hearing loss or between baseline hearing level and cisplatin-induced hearing loss. These findings indicate that cisplatin ototoxicity is independent of age and pre-chemotherapy hearing status of the individuals. We found that a low dose (50 mg/m 2 ) of cisplatin does not affect speech frequencies. However, it affects the higher frequencies (≥4 KHz) as 30% patient were observed to have significant loss at 4-6 KHz, 67% at 8-12 KHz and 57% at 16 KHz. The maximum increase in the hearing threshold after cisplatin administration was 45 dB at 8 KHz in both ears of a 43-year-old patient. This hearing loss was bilateral, symmetrical and sensorineural. These observations were comparable to the study by Laurall et al. , [16] who found hearing loss in 22% patients at 4-6 KHz. Fausti SA et al. [17] reported significant high frequency (>8 KHz) of hearing loss in 71% patients. Cisplatin at 80 mg/m 2 has little effect on lower frequencies; however, hearing impairment starts appearing at> 8 KHz frequencies as hearing loss was observed in 100% cases of Group 2 at> 8 KHz. This observation was comparable to study by Godofredo et al. [18] who, using similar dose, found hearing loss at higher frequencies in seven of eight children. In Group 2, cisplatin caused a maximum increase of 40 dB in the hearing threshold at 12 KHz in the hearing threshold of right ear in a 19-year-old patient. In the left ear, uniform increase of about 30 dB was observed in hearing threshold at all frequencies in all age groups. These observations are suggestive of dose-dependent ototoxicity. Although compared with Group 1 (50 mg/m 2 ), less increase in the hearing threshold was observed at a frequency but ototoxic effect was widespread at 80 mg/m 2 . The hearing loss increased more than 60 dB at the doses of> 80 mg/m 2 (90-100 mg/m 2 ) of cisplatin. We observed significant changes at Fisher′s scale in 66.66% cases. The ototoxicity increased in 91.66% patients at 4-6 KHz and at 8-16 KHz; 100% cases had hearing loss. These observation were comparable to the study done by Laurell et al. , [16] who found significant hearing loss in 81% of 54 patients receiving cisplatin chemotherapy (100-120 mg/m²). A study done by Koplemon et al. [3] found that 1-2 doses of cisplatin (150-225 mg/m²) caused hearing loss in all patients at> 9 KHz and repeated administration of high-dose cisplatin involved lower frequencies also. Cisplatin ototoxicity is symmetrical, progressive, irreversible (follow-up period 3 months) and dose-dependent as hearing loss increases with increase in the dose. CM Schmidt et al. [19] found left-right asymmetry in 55 children after cisplatin. The left ear and boys had more hearing loss compared with the right side and girls. Few authors [20],[21] have found relationship between free circulating cisplatin in plasma with time. They found that cisplatin infusion during afternoon and evening results in low plasma levels of free cisplatin, and hence cisplatin administrated during the early evening hours results in fewer side effects including ototoxicity. Measurement of correlation between time and plasma concentration was beyond the scope of this study. Cisplatin ototoxicity can present with tinnitus. [5],[4],[22] In this study, about six patients had tinnitus irrespective of the dose of cisplatin. The mean age of presentation was 49 years. We found no correlation of tinnitus with the dose of cisplatin or age, which was comparable to the study by Moroso et al . [22] As cisplatin does not affect the vestibular system, [23] none of the patients in this study had any vestibular symptom. The risk of permanent hearing damage from platinum chemotherapy is stimulating the development of otoprotectants for coadministration with platinum to reduce hearing damage without affecting the antitumor activity of the platinum agent. There are numerous otoprotectant agents under research, which include aspirin, antioxidants, [24] intratympanic dexamethasone [25] and hyperbaric oxygen therapy, [26] Ginkgo biloba extract, [27] diethyldithiocarbamate, [28] lipoic acid, [29] adenosine agonist, [30] vitamin E [31] and sodium thiosulfate. [32] Cisplatin isused as a frontline anticancer drug in our Department of Radiotherapy-Oncology (Regional cancer centre). Although, the importance of high-frequency audiometry in cisplatin chemotherapy was established about 25 years earlier, [33] but in majority of the centers including our department, it is used only during research work. However, lack of infrastructure, non-availability of high-frequency audiometer and audiologist is a major problem in these centers, especially in our country. Until we find a substitute of cisplatin, strict protocol of adding high-frequency audiometry in cisplatin regimen should be made so that patients can be alerted for further precautions, e.g., avoidance of noise, ototoxic drugs and trauma. To conclude, we all know that cancer patients are living in physical and mental agony and cisplatin-induced ototoxicity further enhances this morbidity. Audiological monitoring is an essential part of the management of adults and children receiving platinum-based chemotherapy. Although few authors [12],[34],[35] found distortion product otoacoustic emission as a better method of detecting cisplatin-induced early ototoxicity but high-frequency pure-tone audiometry is the first choice due to its high sensitivity. High-frequency monitoring alerts the physician of early ototoxic effects, who has opportunity to change a patient′s course of treatment. Therefore, high-frequency audiometry should be included in the cisplatin-based chemotherapy regimen. Increase in the dose of cisplatin lead to increase in ototoxicity that warrants further research to find therapeutic efficacy of low-dose cisplatin or a better substitute of cisplatin. Otoprotective drugs are still at experimental level but may be beneficial in cisplatin ototoxicity. Acknowledgment Dr RS Minhas provided general help in this research work. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09073f7a.jpg] [cn09073f8c.jpg] [cn09073f8a.jpg] [cn09073f2a.jpg] [cn09073f1.jpg] [cn09073f4a.jpg] [cn09073t2.jpg] [cn09073f8b.jpg] [cn09073f2b.jpg] [cn09073t1.jpg] [cn09073f6a.jpg] [cn09073f4b.jpg] [cn09073f3.jpg] [cn09073f5.jpg] [cn09073f7b.jpg] [cn09073f7c.jpg] [cn09073f6b.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}