 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
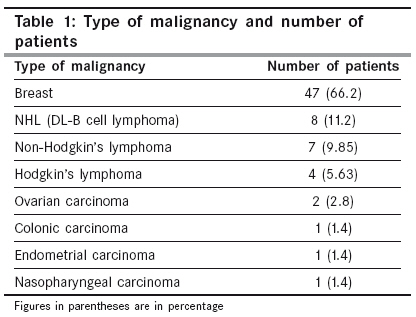
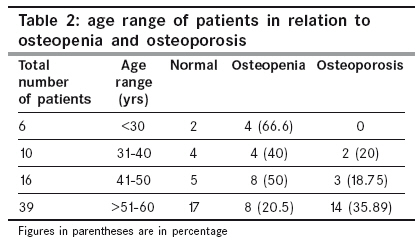
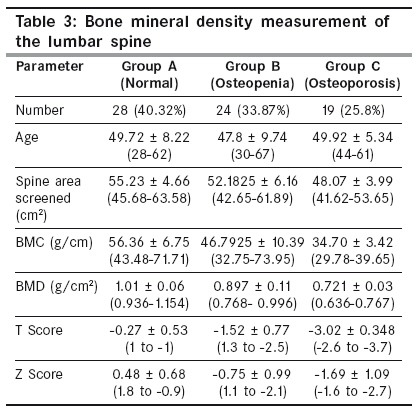
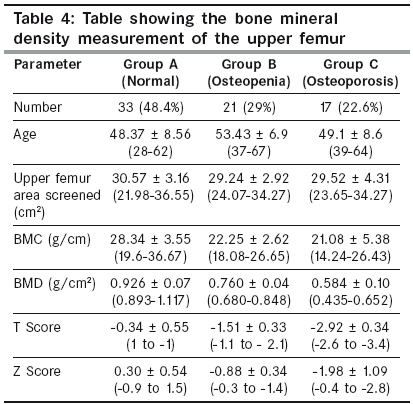
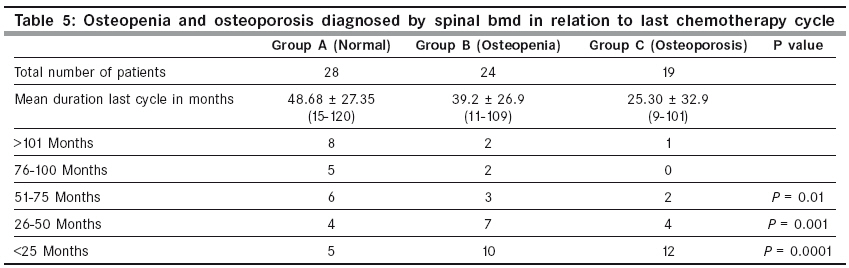
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 331-334 Original Article Cancer chemotherapy-induced osteoporosis: How common is it among Saudi Arabian cancer survivors Al Amri Ali, Sadat-Ali Mir Department of Orthopaedic Surgery, College of Medicine, King Faisal University Dammam and King Fahd University Hospital, Al-Khobar, 31952 Code Number: cn09076 PMID: 19749464 Abstract Objective: This study was done to assess the prevalence of cancer chemotherapy-induced osteoporosis among survivors of cancer in Saudi Arabia.Material and Methods: Patients who received chemotherapy due to malignant disease attending oncology and orthopedic clinics between June 1, 2006 and November 30, 2006, were the subjects. Age, sex, type of malignancy, last chemotherapy cycle and body mass index (BMI) of patients were entered in the database. Complete blood picture, serum calcium, phosphorous, renal function and liver function tests were done. Bone mineral density measurement of the hip and spine was done using Dual-Energy X-ray Absorptiometry. Results: We analyzed the data of 71 patients with an average age of 49.29 ± 8.24 years. Of these, 19 (25.8%) were osteoporotic and 33.87% were found to be osteopenic according to the BMD of the lumbar spine, 17 (22.6%) found to be osteoporotic and 29% found to be osteopenic per the BMD of the hip area. Patients whose BMD was normal had received their last chemotherapy cycle 48.68 ± 27.35 months earlier (P = 0.01). Osteopenia and osteoporosis were more common in patients in the age group of ≤50 years (65.6%) versus 56.4% in patients of ≥51 years (P = 0.001). Patients who received the last cycle of chemotherapy of less than 2 years were significantly more osteoporotic (81.5%-18.5%, P < 0.0001). Conclusions: Our study indicates a high prevalence of osteopenia and osteoporosis in patients who were younger than ≤50 years and who had received cancer chemotherapy. Second, bone loss continued for more than 2 years from the last cycle of chemotherapy. Keywords: Osteoporosis, Osteopenia, Cancer, Chemotherapy Introduction Osteoporosis is characterized by reduction of the bone mass with distortion of the architecture, leading to fractures. Secondary osteoporosis occurs after adjuvant chemotherapy in two-thirds of men, more than half of premenopausal women and about one-fifth of postmenopausal women. [1] Patients with cancer are at increased risk of developing osteopenia and osteoporosis following adjuvant chemotherapy. Cancer Therapy-Induced Bone Loss (CTIBL) is an important cause of secondary osteoporosis, which cause bone fragility and an increased risk of fractures, decreased quality of life and increased mortality. [2],[3] It is estimated that bone loss after cancer chemotherapy can increase up to tenfold higher than normal. [4],[5],[6] With better management and newer drugs for chemotherapy, many patients survive from malignancy but they are faced with a more crippling secondary osteoporosis. [7],[8],[9] Osteopenia and osteoporosis continue to progress without being diagnosed in patients with cancer until a fracture occurs, which leads to increased morbidity and mortality. There is little literature, if any, on the impact of chemotherapy on bone loss among survivors of cancer in Saudi Arabia. With the main objective to assess the prevalence of CTIBL, this retrospective study was conducted to assess the prevalence of bone loss in our patients who had received chemotherapy for cancer. Material and Methods The subjects in this study included patients who had received chemotherapy due to a malignant condition in the last five years. Patients were attending the outpatient oncology and orthopedic clinics between June 1, 2006 and November 30, 2006, were included in the study. The importance of the study was explained to the patients who provided a verbal consent. Age, sex, type of malignancy, last chemotherapy cycle and body mass index (BMI) of patients was entered in the database. Complete blood picture, serum calcium, phosphorous, alkaline phosphatase, renal function tests and liver function tests were done. Bone mineral density (BMD) measurement of the hip and spine was done using Dual-Energy X-ray Absorptiometry (DEXA; Hologic Inc.). Osteopenia and osteoporosis were defined per the definition of World Health Organization. The data were entered in the database and analyzed using SPSS Inc version 14 (Chicago, Illinois). [10] Descriptive statistics are expressed as mean ± SD unless otherwise mentioned. Categorical data were analyzed using χ2 or Fisher′s exact test, as appropriate. A value of P < 0.05 is considered statistically significant. The study was approved by the Research and Ethics Committee of the institution. Results We analyzed the data of 71 patients with an average age of 49.29 ± 8.24 years (range 29-67). [Table - 1] shows number of patients and type of malignancy; 66% of patients suffered from breast cancer. [Table - 2] shows number of patients who were normal, osteopenic and osteoporotic; 19 (25.8%) were osteoporotic and 24 (33.87%) were osteopenic according to the BMD of the lumbar spine [Table - 3] and 17 (22.6%) were osteoporotic and 21 (29%) were osteopenic per the BMD of the hip area [Table - 4]. All osteoporotic patients received the last cycle of chemotherapy of less than mean of 25.30 ± 32.9 months, whereas osteopenic patients received the last cycle 39.2 ± 26.9 months. Patients whose BMD was normal received their last chemotherapy cycle 48.68 ± 27.35 months earlier. Osteopenia and osteoporosis were more common in patients in the age group of < 51 years (65.6%) versus 56.4% in patients of> 50 years ( P = 0.001). Patients who received the last cycle of chemotherapy of less than 2 years were significantly more osteoporotic (81.5%-18.5%; P < 0.0001) [Table - 5]. Discussion Cancer is not uncommon in Saudi Arabia and the National Registry of cancer reported an overall age-standardized incidence for all Saudis Arabian nationals with a world standard reference of 62.6/100,000 (61.6/100,000 in males and 63.5/100,000 in females) for the years 1994-2000, and half of them are over the age of 50 years. [11] It was little anticipated that patients who survive their ordeal of cancer and chemotherapy will face another serious debilitating condition such as secondary osteoporosis. [7],[9] Bone loss after cancer chemotherapy is more rapid in such patients than in normal population between 1% and 5% per year. [12] Bone loss due to cancer therapy should be prevented as bone once lost becomes difficult to regain. Twiss et al . (2001) [13] found that 80% of their patients with breast cancer had abnormal BMD indicating osteopenia or osteoporosis. In this study, we found that even after discontinuation of the chemotherapy 59.67% of patients had abnormal BMD, indicating either osteopenia or osteoporosis. Early detection of osteopenia and osteoporosis by BMD measurement is essential. A recent survey reported that even in the developed countries, 3% to 32% of high-risk patients on cancer therapy had a BMD. [14],[15] In our own institution, a BMD was done in 4.22% of patients before this study was undertaken. It raises serious concern about physicians′ apathy in regular evaluation of patients by BMD. This study shows that even after initial antiresorptive therapy, patients require regular follow-up and correction of their bone loss by multicomponent intervention for postcancer therapy osteoporosis with calcium and vitamin D [16] , physical exercise, lifestyle modification and drugs such as calcitonin, oral or intravenous bisphosphonates and selective estrogen-receptor modifiers (SERMS). [17] Patients with osteoporosis and its related complications has become one of the major causes of morbidity and unprecedented increase in health care budgets in the Western world. The estimated life-time cost of a hip fracture is now increased to $81,300, with an annual budget in the United States increasing to $13 billion. [18] In developing countries, the economic expenses due to postmenopausal osteoporosis and the expenses of secondary osteoporosis such as CTIBL is still to be assessed. Our search of the English language literature did not reveal any reported studies on CTIBL from Gulf countries in general and Saudi Arabia specifically and this retrospective analysis has shown a high percentage of patients with cancer who suffer from osteoporosis due to the effects of their cancer chemotherapy. It will be a pity for these patients to get cured of their malignancies only to succumb to osteoporosis-related fractures with high morbidity and mortality. In conclusion, we believe that patients in postcancer chemotherapy are at a significant risk of increased bone loss. Second, patients need to be monitored with regular BMD measurements to assess the effect of initial antiresorptive therapy. Our results indicate that after cancer chemotherapy not only women but men continued to suffer from osteoporosis. Special efforts are needed to formulate policies to diagnosis and proper treatment of osteoporosis secondary to cancer chemotherapy. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09076t5.jpg] [cn09076t4.jpg] [cn09076t2.jpg] [cn09076t1.jpg] [cn09076t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}