 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
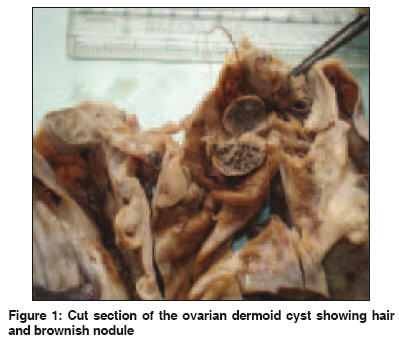
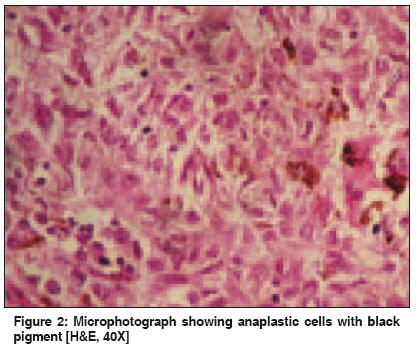
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 340-342 Letter To Editor Primary malignant melanoma in cystic teratoma of ovary Suneja A, Yadav P, Sharma A, Vaid NB, Singh B, Grover RK Department of Obstetrics and Gynaecology, UCMS & GTB Hospital, Delhi Code Number: cn09080 PMID: 19749467 Sir, Primary malignant melanoma of the ovary as a site of metastatic melanoma has been reported in up to 16% of the women, in autopsy studies. [1] Only 31 cases have been reported, including a compilation of 20 cases [1] and individual case reports. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11] A 50-year-old woman, P 3+0+3+3, presented with pain and distension of the lower abdomen for one month. Her present and previous menstrual cycles were normal and there was no other symptom. A general physical examination was apparently normal with no lymphadenopathy. Abdominal and pelvic examination revealed a firm, 20 x 15 cm, smooth, mobile, nontender cystic mass, to the right anterolateral aspect of the uterus. An ultrasound examination showed a right adnexal mass with mixed echogenicity and thin septations, with no ascites or enlarged lymph nodes. The uterus, liver, and other ovary were unremarkable. CA 125 was 53.31 U/ml. Staging laparotomy revealed 100 ml of hemorrhagic ascitic fluid and a 20 x 15 cm right cystic ovarian mass, with solid areas and a smooth capsule. The uterus, left ovary, omentum, liver, bowel, and peritoneum had no obvious lesions. She underwent extrafascial hysterectomy with bilateral salpingo-oophorectomy and infracolic omentectomy. The left ovary, uterus, cervix, and both tubes were unremarkable. The right ovary was converted into a cystic mass 20 x 15 x 12 cm, with a smooth and intact capsule. A cut section revealed a unilocular cyst filled with sebaceous material and hair. The wall was corrugated; 0.2 to 1.0 cm thick and showed a solitary, solid, pigmented, mural nodule, 3 x 3 cm in size [Figure - 1]. On microscopy, a brown nodule and other sections of the tumor were seen to comprise of pleomorphic oval to spindled cells with hyperchromatic nuclei, prominent nucleoli, and frequent mitosis [Figure - 2]. The cytoplasm contained abundant brown pigment, confirmed to be melanin, by its immunohistochemical positivity to HMB-45. On multiple sections, neither the lining epithelium of the cyst nor any intraepithelial junctional activity was detected. No other teratoid tissue of mesodermal or endodermal origin was present in the tumor. Ascitic fluid, omentum, and peritoneal biopsies were negative for malignancy. The histological features and diffuse immunohistochemical expression of HMB-45 favored a diagnosis of melanoma. The patient was re-evaluated and the possibility of a melanoma at any other site, mainly skin, central nervous system, eye, and gastrointestinal tract, was ruled out. Postoperatively she received chemotherapy, using dacarbazine (DTIC) and cisplatin, in the Medical Oncology Department. After one cycle, the patient refused further chemotherapy and died of recurrence in the pelvis and lung metastases, ten months post surgery. Malignant change in a dermoid cyst of the ovary is rare, occurring in 0.2-2% of the cases and squamous cell cancer (SCC) is the commonest change, accounting for 88% of all malignancies. [2] Less commonly, adenocarcinoma, fibrosarcoma, carcinoid tumor, and mixed tumor, in order of decreasing frequency can occur, and malignant melanoma is extremely uncommon and the rarest of all. [1] The present case is a primary malignant melanoma of the ovary, as it meets the criteria laid down by Brought et al . and Croje & Woodruff, that is, it is unilateral, associated with teratoid elements, with no demonstrable extraovarian primary melanoma, and there is good correlation of the patient′s age and symptoms with the well-documented cases in literature. This tumor did not show intraepithelial junctional activity, which is most convincing, although not a mandatory criteria to label it as a primary melanoma of the ovary. This may be due to extensive destruction of the epithelium and the ovarian tissue, by the tumor. Fifty percent of the reported cases do not show junctional activity. [8] The literature consisting of case reports and case series reveals the aggressive behavior of the tumor with 50% survival, at the end of two years. [2],[3],[4],[5],[6],[7],[8],[9],[10],[11],[12] The pattern of the spread is similar to an epithelial ovarian tumor and the prognosis is worse than the squamous cell cancer in a dermoid cyst. [5] The present case was stage IA ovarian cancer and received postoperative chemotherapy, considering the poor prognosis of the tumor. Dacarbazine and platin containing chemotherapy is the most effective for melanoma. [4] Biological and immunotherapy have been used as adjuncts in metastatic melanoma with varying results. It is worth noting that in none of the reported cases a preoperative diagnosis was made or even suspected. It is suggested that if an ovarian cystic teratoma is associated with marked elevation of CA19-9, as well as a low-intensity solid component on T2-weighted MRI, the possibility of malignant melanoma arising in the teratoma should be considered. [7] However, because of the small number of cases in literature, no definite preoperative diagnostic criteria have been laid down. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09080f1.jpg] [cn09080f2.jpg] |
| |||||||||

{kind=link}
{kind=link}