 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
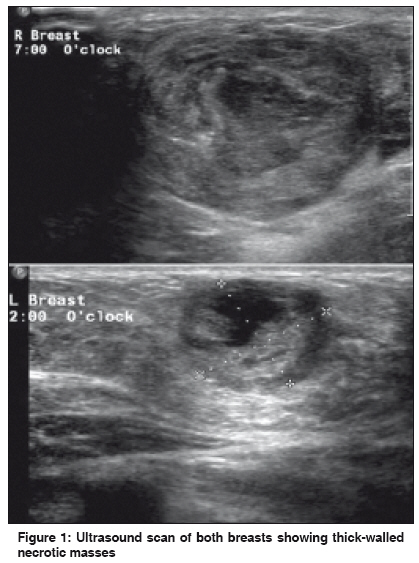
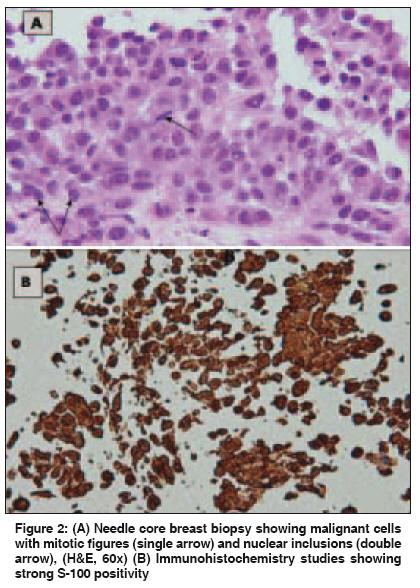
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 342-344 Letter To Editor Bilateral breast metastases in a pregnant woman with disseminated cutaneous melanoma Mathew M, Burney IA, Al Hamadani A, Rao K Departments of Obstetrics and Gynecology, Sultan Qaboos University Hospital, Alkhod, Muscat Code Number: cn09081 PMID: 19749469 Sir, A 28-year-old gravida 2 para 1, at 27 weeks gestation, was referred to us with locally advanced malignant melanoma, for further management. The patient had initially presented with painful left inguinal lymphadenopathy at 12 weeks of gestation. A core biopsy from the lymph node showed a totally effaced architecture by malignant cells consisting of poorly differentiated round to oval tumor cells, arranged in vague irregular nodular masses. Some of the cells showed a large ovoid nucleus with deeply eosinophilic cytoplasm, others were spindly with epitheloid-like cells and large areas of necrosis. The stroma showed fibrous septa with inflammatory cell infiltration. The diagnosis was suggestive of malignant high-grade neoplasm. Immunohistochemistry showed positive staining, with S-100, Melanin A, and Vimentin confirming malignant melanoma. Examination at our institution showed a left inguinal mass, dark-colored, measuring 10 x 7 cm, extending from the left anterior superior iliac spine to the pubic symphysis. This mass was lobulated, mostly solid, with some cystic component. A complete physical examination revealed a raised nevus 8 x 7 mm in size with satellite lesions in the upper lateral part of the left thigh. Both breasts had mobile, nontender, firm masses mimicking fibroadenoma: 3 x 3 cm in the right breast and 2 x 1 cm in the left breast. After multidisciplinary evaluation by an oncologist, neonatologist and obstetricians, labor was induced at 28 weeks of gestation, resulting in a male baby weighing 1310 gm. Gross as well as histological examination of the placenta did not show any metastasis. There were no signs of disease in the newborn. Lactation was suppressed using Cabergoline. Metastatic workup soon after delivery revealed extensive involvement of lungs, liver, spleen, and both breasts. [Figure - 1] shows the mammographic appearance of right and left breast lumps. Needle core biopsy and immunohistochemistry of the breast lumps confirmed metastatic melanoma [Figure - 2]. MRI of the brain did not show any metastasis. The patient was started on palliative chemotherapy with Cisplatin, Vinblastine, and Dacarbazine. The disease progressed and the patient died four months after delivery. Metastatic breast disease may be difficult to differentiate from primary breast carcinoma, leading to extensive surgery and a delay in the appropriate treatment. [1],[2] Melanoma is one of the most common primary tumors to metastasize to the breasts. Other sources of breast metastasis include, lymphomas, lung cancer, rhabdomyosarcoma, renal cancer, ovarian cancer, and gastrointestinal cancer. [2],[3] Bilateral breast metastasis with malignant melanoma during pregnancy is extremely rare. Metastatic tumors of the breast are often misdiagnosed as primary breast malignancies, which may lead to a delay in the appropriate treatment. [2] Usually breast metastasis presents as a well-circumscribed mass. In a majority of the reported cases the metastatic tumor mass remained pain-free. [3] Melanoma metastasizing to the breast may be indistinguishable from a fibroadenoma, clinically and ultrasonographically. [4] The mammographic appearance of breast metastasis is usually specific, to differentiate it from a primary. Usually, they are well-circumscribed masses without any visible microcalcifications. Nipple discharge is usually absent. [3] In our case the breast lumps were discrete, firm, mobile, pain-free, and there was no nipple discharge. Breast metastasis may be the initial presentation of a widely metastatic melanoma. [5] Once suspected on imaging or fine needle aspiration biopsy, histology with immunohistochemistry confirms the diagnosis. The treatment of metastatic breast tumors depends on the extent of the disease, the intended treatment of melanoma, and a wide local excision is usually sufficient. [1] An autopsy series of patients with melanoma metastatic to the breast showed that the patients were considerably younger than those with other tumors. Several explanations have been suggested for melanoma metastasizing to breast in the young. It is plausible that there is an increased blood flow and hence a higher chance of metastasis. The predilection for metastatic spread to the breast in premenopausal women may be due to direct lymphatic and vascular drainage. A hormonally based association is suspected because estrogen receptors have been detected in melanoma tissue, although in low levels and infrequently. [1],[6] A review of the published series of melanoma with metastasis to the breast shows that the most common sites of the primary melanoma, in premenopausal women, are the arms and the trunk, whereas, generally the most common site of primary melanoma is the lower extremities. [5],[6] Our patient had bilateral breast metastasis with the primary over the left thigh. Ravdel et al., [6] have reported a series of 27 cases of breast metastasis from melanoma. Twenty (77%) were premenopausal females with a mean age of 41.4 years. The majority of patients had primary lesions on the upper body; only four had a primary in the lower extremity. The median interval between diagnosis of the primary melanoma and breast involvement was 52.5 months (range 1-192 months) and the median survival after diagnosis of breast metastases was 12.9 months (range 2-37 months). The overall prognosis of patients with malignant melanoma metastatic to the breast is poor, as it is usually associated with the disseminated disease. In our case the disease progressed rapidly in spite of combination chemotherapy and the patient passed away within four months of the diagnosis of breast metastasis. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09081f2.jpg] [cn09081f1.jpg] |
| |||||||||

{kind=link}
{kind=link}