 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
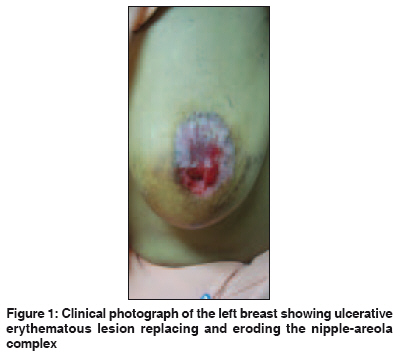
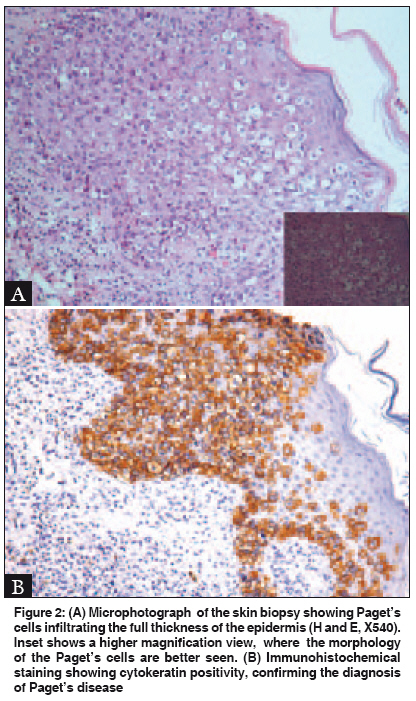
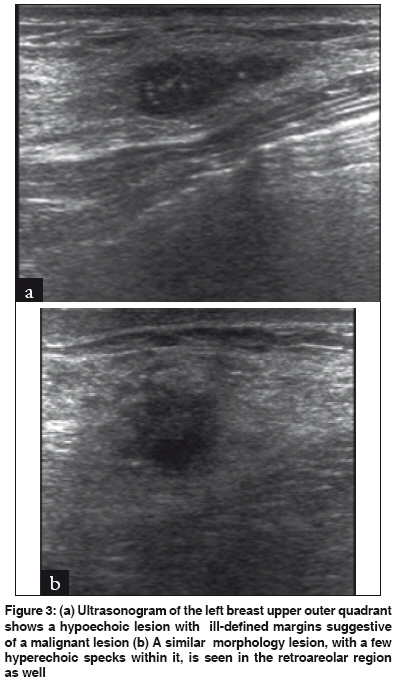
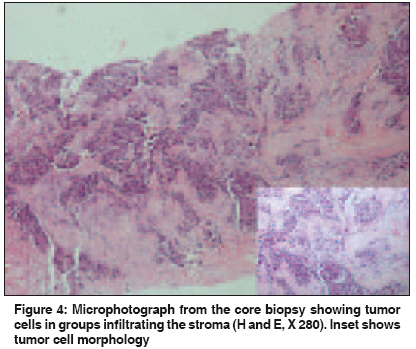
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 344-347 Letter To Editor Paget's disease of breast masquerading as chronic benign eczema Singla V, Virmani V, Nahar U, Singh G, Khandelwal NK Department of Radiodiagnosis, PGIMER, Chandigarh Code Number: cn09082 PMID: 19749470 Sir, Paget′s disease of the breast is an uncommon form of breast cancer and comprises 1-4% of all mammary tumors. [1] In this condition, infiltration of the nipple epidermis by adenocarcinoma cells causes chronic eczematous eruptions on the nipple and areola. We report a case of Paget′s disease of the nipple, with underlying multicentric carcinoma, which was initially misdiagnosed as benign eczema and treated with topical steroids. This case highlights the clinical, radiological, and histological features of this uncommon disease, awareness of which is essential to prevent delayed therapy. A 24-year-old female presented to the out-patient services of our institute with an ulcerative lesion that had completely effaced the nipple and areola of the left breast [Figure - 1]. The lesion had started as a scaly plaque involving the nipple and areola one year back, for which she was treated with topical steroids by a local physician. Subsequently over a period of the last two months, the lesion had rapidly progressed to cause ulceration and nipple deformity. On clinical examination, a well demarcated erythematous lesion was seen distorting the nipple-areola complex, extending into the surrounding skin. A firm, nontender, nonmobile lump could be palpated in the upper-outer quadrant of the breast. No lymph nodes were palpable. A skin biopsy from the region of the nipple and areola was taken and subjected to histopathology. The tissue was routinely processed for Hematoxylin and Eosin stain. A light microscopic examination showed acanthotic epidermis and prolonged rete pegs. There was a presence of large round cells, with moderate-to- abundant pale staining cytoplasm, permeating singly and in groups in all layers of the epidermis [Figure - 2]. The nuclei were vesicular with prominent nucleoli in some of them. Immunohistochemical staining showed strong carcinoembryonic antigen (CEA) positivity within the cytoplasm, thereby confirming the diagnosis of Paget′s disease. An ultrasonogram revealed hypoechoic mass lesions in the retroareolar and 2 o′clock positions, with a few small hyperechoic internal specks, suggestive of foci of microcalcification, suggesting lesions suspicious for malignancy [Figure - 3]a, b. A core biopsy from these masses revealed features of infiltrating ductal carcinoma with features of high grade tumor [Figure - 4]. A diagnosis of Paget′s disease of the nipple with underlying multifocal infiltrating ductal carcinoma was established. The metastatic workup of the patient, including a bone scan, was negative. The decision of modified radical mastectomy was taken. The postoperative period was uneventful and the patient is currently asymptomatic after a follow-up of nine months. Paget′s disease of the breast is a distinct entity comprising of well-marginated erythema and scaling of the nipple-areola complex, which is often a harbinger of an underlying breast neoplasm. Paget′s disease can have three different presentations (1) in conjunction with invasive cancer (2) with underlying ductal carcinoma in situ [DCIS], or (3) alone without underlying invasive cancer or ductal carcinoma. [2] There are two different theories proposed for the origin of Paget′s disease. The epidermotropic theory holds that Paget cells arise in the main secretory ducts of the breast and migrate from the underlying breast parenchyma to involve the skin of the nipple, and this is supported by the fact that the incidence of underlying carcinoma has been reported to be as high as 90-100% in most series. [3] The in situ transformation theory, propounded to explain the small number of cases without underlying mammary carcinoma, states that the Paget cells arise as malignant cells in the epidermis of the nipple and areola, independent of the underlying carcinoma, by means of in situ malignant transformation or degeneration of the existing cells. [3] The age range is 24-84 years with the mean age of diagnosis being 55 years. [4] The clinical features suggestive of the disease include erythema and scaling or eczematous changes in the nipple, which may later progress to ulceration, erosion and frank destruction, bloody nipple discharge, nipple retraction, or a palpable mass. These features may initially result in missing of the correct diagnosis and the condition may simulate benign eczema, psoriasis, or dermatitis resulting in treatment with topical steroids, as in the index case. The reported median delay in diagnosis is about 6-11 months. [1] Although mammograms have been reported to be positive in only 40-50% of the cases, they may detect the underlying tumor in certain cases. Classically the underlying carcinoma is invasive in nature, although in 40-45% of the cases, the underlying pathology is ductal carcinoma in situ (DCIS). [4] A multifocal or multicentric mass may be found in 32-41%. [4] An MRI may be useful in detecting occult, mammographically negative breast carcinomas in Paget′s disease. The histological hallmark of Paget′s disease is the involvement of the epidermis by malignant Paget cells, having abundant clear or pale staining eosinophilic cytoplasm and nucleoli with intracytoplasmic vacuoles. [5] On immunohistochemistry the Paget cells are positive for CEA and CK7 (specific and 100% sensitive markers for mammary Paget′s disease), helping to differentiate it from keratinocytic tumors such as Bowen′s disease (squamous cell carcinoma in situ of the breast). [5] The other differential diagnosis includes malignant melanoma, where the cells are quite large with prominent eosinophilic nucleoli. The melanoma cells are, however, positive for S-100 protein and HMB-45 and their negativity for CEA on immunohistochemistry helps to differentiate them from Paget cells. Paget cells express HER2 / NEU receptors and the c-erb B-2 oncogene, further confirming a common histological and biological origin with the underlying breast carcinoma. [5],[6] Mastectomy, with or without axillary node dissection, has been the standard treatment for Paget′s disease. Of late, a more conservative approach, based on clinical and mammography findings has been adopted. [7],[8] Breast conservation surgery is recommended in cases where the disease is diagnosed early enough and the cancer has not spread far from the surface of the nipple. However, presence of the underlying multifocal, invasive cancer precluded conservative surgery in the index case and modified radical mastectomy was opted for. Controversies regarding selection of surgical procedure continue to exist with proponents of mastectomy citing the high frequency of occult cancer identified in surgical specimens. Nonetheless, patients who undergo conservative breast operations have been reported to have therapeutic outcomes similar to those undergoing mastectomy. [2] If the patient has a palpable mass, segmentectomy along with tissue sampling from adjacent quadrants and axillary node dissection can be performed. [8] In case the margins are positive, then total mastectomy with axillary clearance should be performed. Adjuvant chemoradiotherapy, if given, is based on several factors that include patient′s age and nodal status. [7] This case highlights the importance of doing an early skin biopsy in innocuous looking breast lesions. Persistence of eczematoid lesions on the breast for more than two weeks should be viewed with suspicion and warrant thorough evaluation, including mammography. In conclusion, Paget′s disease remains an elusive clinical diagnosis due to its varied presentations, ranging from change in sensation, itching, and burning, to ulceration and destruction of the nipple-areola complex. Awareness of the clinical presentation and pathogenesis of this uncommon condition alerts the clinician to search for underlying carcinoma, which facilitates early detection and treatment, with better prognosis. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09082f1.jpg] [cn09082f3.jpg] [cn09082f4.jpg] [cn09082f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}