 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
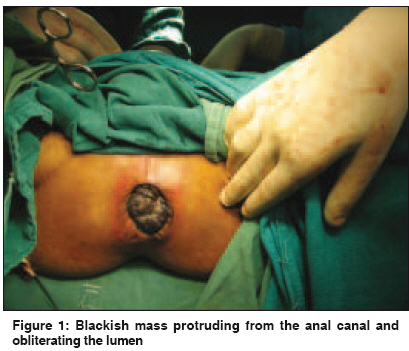
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 347-348 Letter To Editor Primary malignant melanoma of anorectum: A rare entity Jayant M, Agarwal PN Department of Surgery, Maulana Azad Medical College and Associated Lok Nayak Hospital, New Delhi Code Number: cn09083 PMID: 19749471 Sir, Melanoma of anus and / or rectum is a rare but highly malignant tumor with poor prognosis. This disease is often mistaken for benign diseases, such as, hemorrhoids or rectal polyps, as they are the most common causes of bleeding per rectum. [1] Because the disease is very uncommon, the treatment is not well defined. The response of anorectal melanoma to radiotherapy and chemotherapy is poor and optimum surgical treatment is controversial. A 60-year-old man presented with complaints of bleeding per rectum and protrusion of a mass during defecation for the last 10 months. He also developed pain during defecation over the last four months, with loss of weight and appetite. The patient was being treated for piles for the last seven months by some general practitioner. On examination, the general condition of the patient was poor, pallor was evident, but there was no inguinal lymphadenopathy. Abdominal examination was normal. Perianal examination showed a blackish mass protruding from the anal canal on straining [Figure - 1]. Per rectally, there was a fragile growth present about 2 cm from the anal verge, which almost completely obliterated the rectal lumen. The upper limit of the growth was not palpable. A bunch biopsy was taken, which revealed malignant cells with abundant melanin pigment. Hence a diagnosis of malignant melanoma was made. All biochemical investigations including liver function tests and renal function tests were within normal limits, except that the patient was anemic, Hb - 6.5 gm%. Enzyme-linked Immunosorbent Assay (ELISA) for Human Immunodeficiency Virus (HIV) and hepatitis B surface antigen (HBsAg) were negative. A computed tomography (CT) scan showed a mass arising from the wall of the rectum, which was almost obliterating the lumen of the anorectum. There was no mesenteric lymphadenopathy, ascitis or liver metastasis. Perirectal fat planes were well preserved. Considering these findings the growth was deemed operable and the patient was taken up for surgery. An abdominoperineal resection was carried out. The resected mass was 10 x 8 cms and an on-cut section revealed a blackish mass [Figure - 2]. The final histopathological report was consistent with diagnosis of malignant melanoma with no regional lymph node metastasis. The patient is under follow up and is doing well with no symptoms of metastasis for the last six months. No adjuvant therapy has been started on the patient. Malignant melanoma of the anorectum is a rare condition. Primary anorectal melanoma comprises 0.25 % to 1.25% of all the malignancies in this anatomical region. [2] Of all the melanomas, anorectal melanoma represents less than 2% and is the third most common site following the skin and eye. It is usually a disease of old age affecting mostly in the seventh decade of life with no sex predilection. [3] The initial symptom of presentation is bleeding per rectum, and the patient may delay consultation assuming symptoms to be hemorrhoidal disease. [4],[5] Surgery remains the mainstay of the treatment, but the surgical therapy is uncertain and controversial. Surgical management includes a conservative approach of wide local excision (WLE) of the tumor or a more radical approach of abdominoperineal resection (APR). Thibault et al. reviewed the literature comparing WLE and APR as treatment modalities for anorectal melanoma and concluded that there was no difference in the survival rates after five years in both the groups, but the incidence of local recurrence was notably higher in the WLE group as compared to the APR group (47% vs. 23%). [6] Poor prognosis was evident in all the series reviewed and the mean survival was 29 months, irrespective of the surgical procedure performed. [5] Poor survival of the anorectal melanoma patients can be attributed to the relative aggressiveness of the tumor. The most important predictors of prognosis are stage of disease, duration of symptoms,size of tumor and nodal status. [4] Surgical decision must therefore be individualized according to the severity of the local symptoms, presence of the distant metastasis, and the overall well being of the patient. The goal of therapy should be to maximize both the quality and the quantity of life and minimize morbidity. Adjuvant chemotherapy and radiotherapy have not added to any advantage regarding the survival or recurrence rates. Although adjuvant radiotherapy is being used sparingly, it needs large patient data or a multicenter study to prove its efficacy. [5] As anorectal malignant melanoma is frequently advanced at the time of diagnosis, an early diagnosis is critical to reduce the mortality rate. In our case, the growth that was present 2 cm from the anal verge and was about 10 cm long, making it unsuitable for a wide local excision, therefore, an abdominoperineal resection was performed. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09083f1.jpg] [cn09083f2.jpg] |
| |||||||||


{kind=link}
{kind=link}