 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
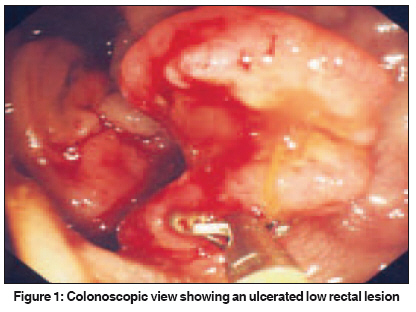
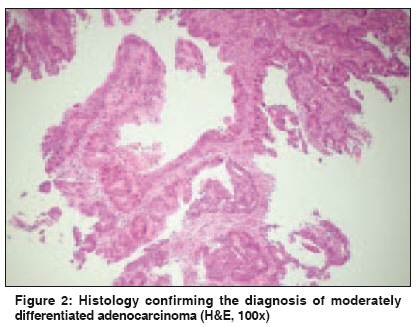
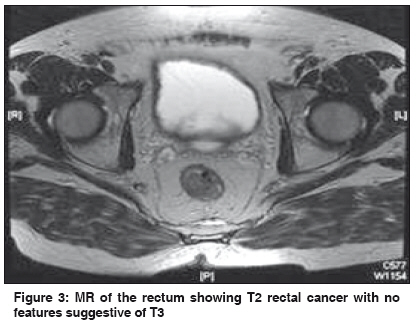
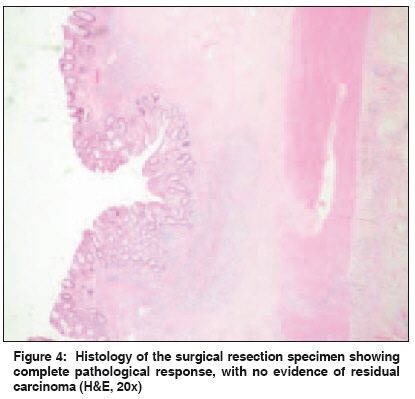
Indian Journal of Cancer, Vol. 46, No. 4, October-December, 2009, pp. 350-351 Letter To Editor Complete clinical and pathological response to preoperative short course radiotherapy in T 2 rectal cancer Selvasekar CR, Obeidat S, Simcock P, Khan AU Department of Surgery, Leighton Hospital, Crewe, CW1 4QJ Code Number: cn09085 PMID: 19749473 Sir, Radical surgery including total mesorectal excision (TME) is the treatment of choice for localized rectal cancer. [1] Nevertheless, despite optimal surgery, local recurrence is around 20%, which is reduced to less than 5% with TME and neoadjuvant treatment. [2] Neoadjuvant short-course radiotherapy (SCRT) for rectal cancer is used to decrease local recurrence [2],[3] and improve an overall and disease-free survival. [3] Recently, we had a 70-year-old male with rectal cancer treated with SCRT, where a complete clinical and pathological response was demonstrated. He was noted to have an ulceroproliferative tumor 4 cm from the anal verge [Figure - 1]. A colonoscopy and biopsy confirmed moderately differentiated adenocarcinoma [Figure - 2]. Magnetic resonance imaging (MRI) of the pelvis showed the lesion to be T 2 N 0 [Figure - 3] with no evidence of metastasis. The patient underwent SCRT followed by abdominoperineal excision of the rectum and anus 19 days later. Macroscopically, there was normal mucosa, and seven lymph nodes were identified. Histology showed features in-keeping with the previous radiotherapy, characterized by focal transmural fibrosis and a patchy transmural chronic inflammatory infiltrate. No residual neoplasia was identified and all lymph nodes showed simple reactive changes [Figure - 4]. Surgery remains the mainstay treatment for rectal cancer, [1] although in Europe radiotherapy has been used in the neoadjuvant and adjuvant setting for a long time, to reduce local recurrence. [4] Short course radiotherapy (SCRT) including the Dutch Colorectal Cancer Group and the Swedish Rectal Cancer Trial demonstrated a reduced risk of local recurrence [2],[3] and concluded that preoperative SCRT might improve survival among patients with resectable rectal cancer. [3] In both these trials surgery was performed within a week of completing radiotherapy. A randomized controlled trial from Poland showed no difference in the local recurrence rate or survival and toxicity rate when comparing SCRT and CRT, which suggests an intensive radiotherapy protocol is achieved with SCRT. SCRT achieves similar results as those by the prolonged standard CRT. [5] In our patient there was a delay of 19 days before radical surgery was performed. This could have contributed to the complete pathological response. There is reasonable literature on chemoradiation producing 15-30% complete pathological response [4] and this response may be increased with increased time delay between neoadjuvant treatment and surgery, [6] but this evidence is not conclusive. There is some evidence that the subgroup of patients who have favorable tumor regression grade and lymph node status may have a higher rate of complete response. [7] There is an American College of Surgeons Oncology Group (ACOSOG)-supported prospective trial in progress, using local excision following chemoradiation for ultrasound staged T 2 distal rectal cancer. [8] In a significant proportion of a high-risk patient′s neoadjuvant treatment, either SCRT or CRT may result in a complete response, whereby, major rectal cancer surgery may be avoided or a local excision with minimal morbidity can be performed. To test this hypothesis, there is a need for a multi-arm randomized controlled trial of early rectal cancer, that is, < = T2 with no nodal disease on radiological staging, receiving SCRT or CRT with varying periods between radiotherapy and radical surgery, to define the optimal time period between radiotherapy regimes and surgery and to find the subgroup of patients where a major resection can be avoided. References
Copyright 2009 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn09085f3.jpg] [cn09085f2.jpg] [cn09085f4.jpg] [cn09085f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}