 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
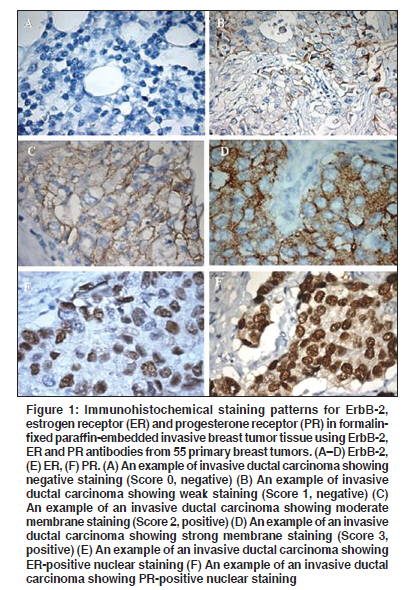
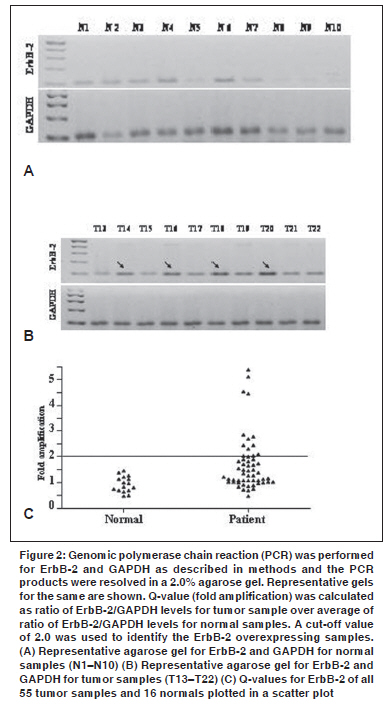
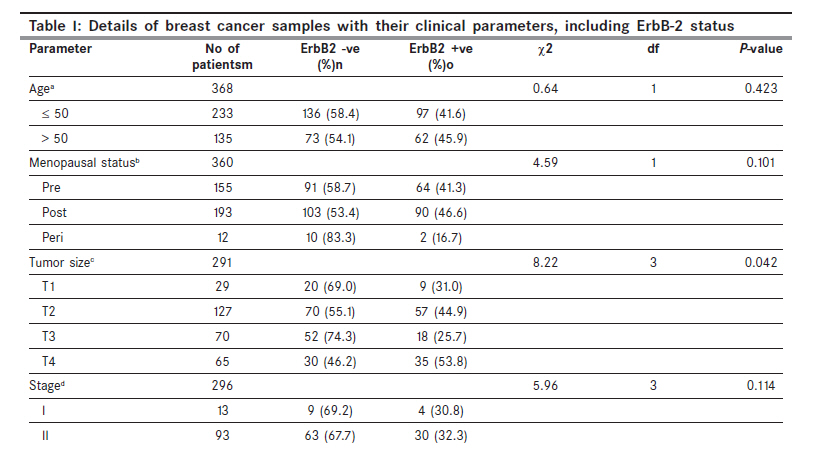
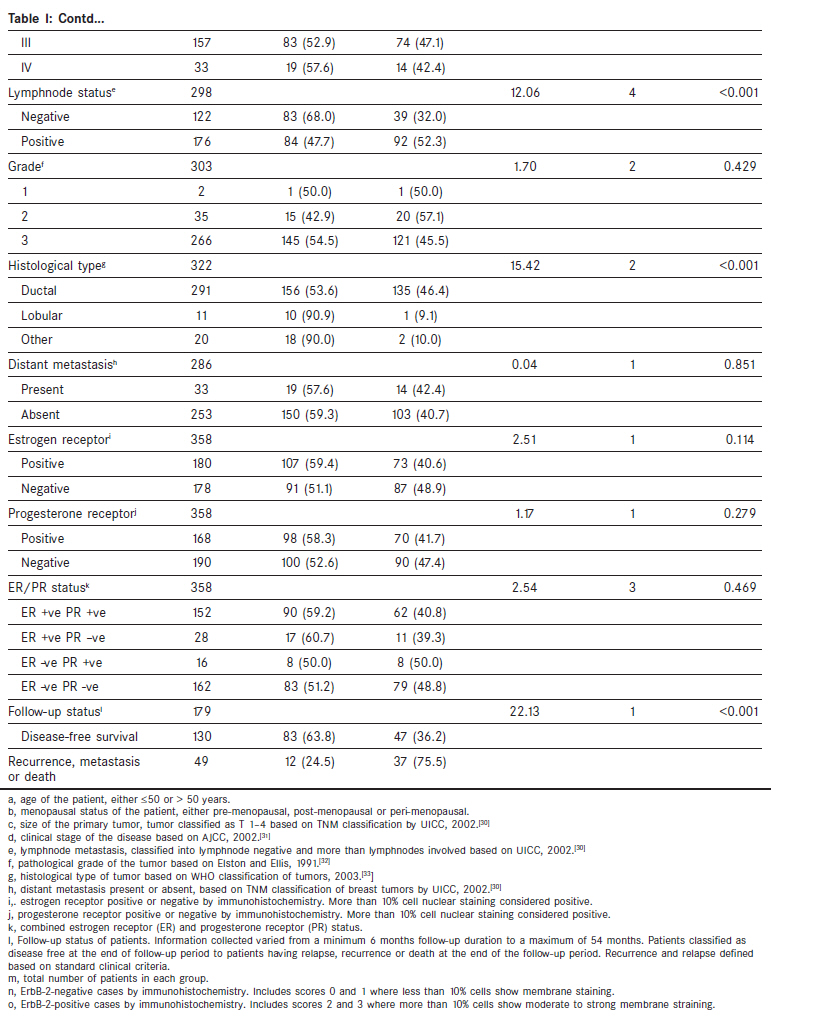
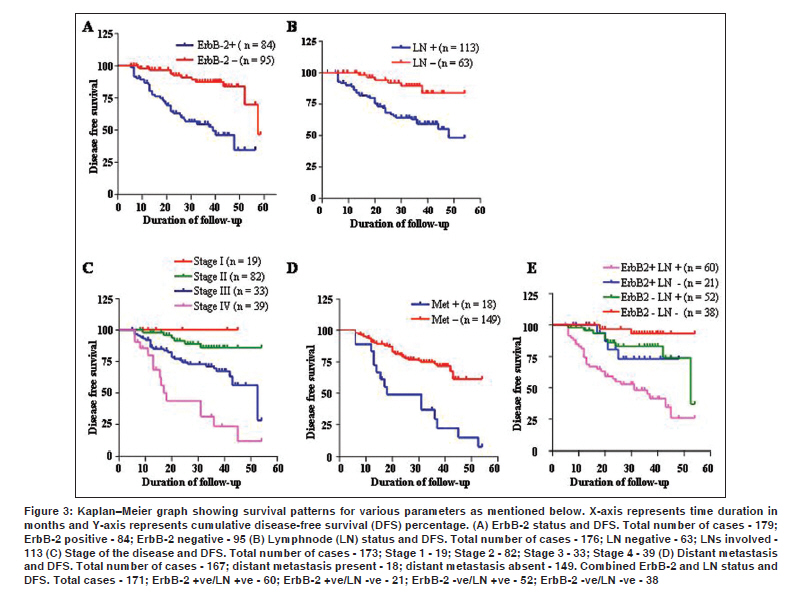
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 8-15 Original Article ErbB-2 expression and its association with other biological parameters of breast cancer among Indian women Vaidyanathan K, Kumar P1 , Reddy CO1 , Deshmane V2 , Somasundaram K, Mukherjee G1 Department of Microbiology and Cell Biology, Indian Institute of Science, Bangalore - 12, Departments of 1 Pathology and 2 Surgery, Kidwai Memorial Institute of Oncology, Bangalore - 68, India Code Number: cn10004 PMID: 20071783 DOI: 10.4103/0019-509X.58852 Abstract Objectives: Overexpression of the epidermal growth factor receptor family genes, which include ErbB-1, 2, 3 and 4, has been implicated in a number of cancers. We have studied the extent of ErbB-2 overexpression among Indian women with sporadic breast cancer. Methods: Immmunohistochemistry and genomic polymerase chain reaction (PCR) were used to study the ErbB2 overexpression. ErbB2 status was correlated with other clinico-pathological parameters, including patient survival. Results: ErbB-2 overexpression was detected in 43.2% (159/368) of the cases by immunohistochemistry. For a sub-set of patients (n = 55) for whom total DNA was available, ErbB-2 gene amplification was detected in 25.5% (14/55) of the cases by genomic PCR. While the ErbB2 overexpression was significantly higher in patients with lymphnode (χ2 = 12.06, P≤ 0.001), larger tumor size (χ2 = 8.22, P = 0.042) and ductal carcinoma (χ2 = 15.42, P ≤ 0.001), it was lower in patients with disease-free survival (χ2 = 22.13, P ≤ 0.001). Survival analysis on a sub-set of patients for whom survival data were available (n = 179) revealed that ErbB-2 status (χ2 =25.94, P ≤ 0.001), lymphnode status (χ2 = 12.68, P ≤ 0.001), distant metastasis (χ2 = 19.49, P ≤ 0.001) and stage of the disease (χ2 = 28.04, P ≤0.001) were markers of poor prognosis. Conclusions: ErbB-2 overexpression was significantly greater compared with the Western literature, but comparable to other Indian studies. Significant correlation was found between ErbB-2 status and lymphnode status, tumor size and ductal carcinoma. ErbB-2 status, lymph node status, distant metastasis and stage of the disease were found to be prognostic indicators.Keywords: Breast cancer ErbB-2, genomic polymerase chain reaction, immunohistochemistry Introduction ErbB-2 is a transmembrane growth factor receptor belonging to the type I receptor tyrosine kinase family of proteins. It is related to epidermal growth factor receptor (EGFR) and has high homology with other members of the EGFR family, which include ErbB-1, ErbB-3 and ErbB-4 as well. [1],[2] The gene is located on chromosome 17q21 and encodes a 185 kDa protein. [3] It has 1255 amino acids and is a highly phosphorylated protein. Normally, ErbB-2 is expressed in a wide variety of tissues and is involved in normal growth, cell adhesion and development. ErbB-2 can both homodimerize and heterodimerize with other members of the EGFR family and activates a range of signal transduction pathways. [4],[5] ErbB-2 is an oncogene and is found to be overexpressed in 25-30% of sporadic breast cancers. [6],[7],[8] It is important to study whether ErbB-2 is overexpressed in breast cancer patients because these patients can opt for herceptin therapy, which is highly efficient for these patients. [9] Breast cancers overexpressing ErbB-2 are resistant to conventional therapy. They are also found to be more aggressive tumors compared with those that are negative. [9] It is also found that ErbB-2-positive tumors also frequently have tumor metastasis to lymph nodes. [10],[11] Estrogen receptor (ER) and progesterone receptor (PR) are expressed in 70-80% and 60-70% cases of invasive ductal carcinoma, respectively. [12],[13] Patients with higher levels of ErbB-2 overexpression or amplification had statistically significant lower levels of ER/PR than patients with lower levels of ErbB-2 overexpression or amplification. Because absolute HR levels are strongly related to response to hormone therapy in primary and advanced breast cancer, reduced ER/PR expression may be one mechanism to explain the relative resistance of ErbB-2-positive:HR-positive tumors to hormone therapy. [14] Mechanisms involved in ErbB-2 overexpression include gene amplification and increased transcription, which in turn lead to increased protein turnover. [15] Gene amplification is known to be one of the major mechanisms responsible for ErbB-2 overexpression. The objectives of the present study are: (1) to study the incidence of ErbB-2 overexpression in Indian sporadic breast cancer patients and (2) to correlate the ErbB-2 expression with various clinico-pathological parameters, including patient survival. Materials and Methods Fifty-five consecutive breast tissue samples were collected from patients (study period 2004-2005) in the Department of Pathology, Kidwai Memorial Institute of Oncology, Bangalore, at the time of surgery and stored at -80 o C. Samples were transported to the laboratory in ice and stored again at -80 o C until use. Relevant details about patients were collected at the time of surgery itself. Sixteen normal samples were collected from healthy breast tissue in patient samples. Only 16 normal samples were available for inclusion in the study. Patients selected had not undergone treatment before surgery. We also included 313 patients for whom paraffin blocks were available, who were admitted to the hospital during the years 1999-2002 for immunohistochemistry. One hundred eighty control paraffin blocks were included for immunohistochemistry. All patients underwent surgery (modified radical mastectomy, lumpectomy or toilet mastectomy) followed by radiation therapy and chemotherapy. Patients underwent four cycles of adriamycin and cyclophosphamide (AC regimen). All patients who were ER positive had also undergone tamoxifen therapy. Some patients had also taken adjuvant therapy. All patients with family history of breast cancer were excluded. Informed consent was obtained from all patients involved in the study. Study protocol was approved by the ethical committee. The period of study is from 1999 to 2005. Genomic DNA was extracted from the breast cancer tissue samples using a DNA extraction minikit (Qiagen, Germany) following the manufacturer's protocol. DNA was quantitated using a Nanodrop spectrophotometer (Nano Drop Technologies, USA) and stored at -80°C. MyCycler (BioRad, USA) was used for performing the polymerase chain reaction (PCR). PCR was performed for GAPDH using 4 ng total DNA. [16] Conditions for GAPDH were initial denaturation at 95 o C and 35 cycles of denaturation at 95 o C for 1 min, annealing at 50.3 o C for 1 min and extension at 72 o C for 45 s followed by a final extension at 72 o C for 7 min. PCR conditions for ErbB-2 amplification were 30 cycles of denaturation at 95 o C for 45 s, 56 o C annealing for 45s and extension at 72 o C for 30 s followed by a final extension at 72 o C for 7 min. PCR products were separated on 2% agarose gels for further visualization and quantitation. The fold amplification (Q-value) was calculated as the ratio of ErbB-2/GAPDH for each sample (patient, p, or normal, n) to that of the average of the same ratio for normal controls (na). i.e., Q = ErbB-2 p (n) /GAPDH p (n) ErbB-2 na /GAPDH na To determine the ErbB-1/2 overexpression, cut-off was taken as 2.0. [16] Primers used in the study were GAPDH (F - 5'-CATGTTCCAATATGATTCCA C-3' and R - 5-CCTGGAAGATGGTGATG-3) and ErbB-2 exon 20 (F- 5'-GAA CTGGTGTATGCAGATTGC-3' and R- 5-AGCAAGAGTCCCCATCCT A-3). Primers were obtained from Sigma Chemicals and were manufactured in Bangalore, India. Of the 368 patients for whom ErbB-2 immunohistochemistry was performed, survival information was available for 179 patients. Inclusion of these patients was not based on any criteria. Follow-up duration ranged from 6 months to 4.5 years. Kaplan-Meier plots were generated for the survival analyses. Graph Pad Prism 4.0 software was used for Kaplan-Meier graph plotting and calculation of P-values, χ2 and degree of freedom. In all cases, only P-values less than 0.05 were considered significant. Graph Pad Prism 4.0 software was also used for statistical analysis for comparison of ErbB-2 status with other parameters. Immunohistochemistry for ErbB-2 was carried out using antibody from Novocastra, UK (Cat No: NCL-L- CBE-356). Briefly, 5 m paraffin-embedded tissue sections were deparaffinized and rehydrated in two changes of xylene, 5 min each and 100% alcohol, 3 min two changes each and rinsed in distilled water twice. Antigen retrieval was performed in a water bath at 98 o C for 40-45 min using antigen retrieval solution provided diluted 1:10. After cooling to room temperature for 20 min, slides are again rinsed in distilled water twice. Peroxidase blocking was carried out using 3% hydrogen peroxide for 5 min. Slides were washed in wash buffer for 5 min twice. Primary antibody (1:80 dilution) was added and incubated for 2 h. Secondary antibody incubation was carried out for 30 min. Slides were again washed in wash buffer for 5 min twice and treated with visualization reagent for 30 min. After washing in wash buffer for 5 min twice, diamino benzidine was added for 10 min. Slides were counterstained in hematoxylin, rinsed in distilled water and viewed under a microscope. Staining was performed in a humidified chamber. Positive and negative controls were used in each case. Strong membrane staining in more than 10% of the tumor cells is taken as strongly positive (Score 3). A weak to moderate complete membrane staining in more than 10% of the tumor cells is taken as weakly positive (Score 2). A faint, barely perceptible membrane staining detected in more than 10% of the tumor cells is negative (Score 1). No staining or staining in less than 10% of the cells is negative (Score 0). Immunohistochemistry was performed following the HercepTest protocol by Dako Corporation, Denmark. ER and PR staining were carried out using antibodies from Novocastra (Cat No: ER - NCL-ER-6S11 and PR - NCL - PGR). Antigen retrieval was carried out in a pressure cooker. Other steps of the procedure are similar to that described for ErbB-2. Nuclear staining in more than 10% of the cells was considered as positive for both ER and PR. Results We first investigated the status of ErbB-2 by immunohistochemistry. Of 368 paraffin block sections analyzed, 43.2% (159/368) of the cases were found to be positive (Score 2 or 3; [Figure - 1]C and D respectively). Of the ErbB-2-positive cases, a majority (151/159) of them had Score 3. For a sub-set of 55 breast cancer samples, for which total DNA was available, ErbB-2 status was analyzed by genomic PCR as well. Surprisingly, we found that only 25.50% (14/55) of the samples had increased on ErbB-2 gene amplification [Figure - 2]A-C. We analyzed the correlation between ErbB-2 status and various clinico-pathological parameters. ErbB-2 overexpression was found to positively correlated with lymphnode status, tumor size and ductal carcinoma [Table - 1]. It was found that there was no appreciable correlation between ErbB-2 status and patient age and menopausal status, tumor grade, distant metastasis or stage of the disease [Table - 1]. With regard to lymphnode status, 52.3% (92/176) lymphnode-positive cases were ErbB-2 positive while only 32.0% (39/122) lymphnode-negative cases were ErbB-2 positive (χ2 = 12.06, P ≤ 0.001). ErbB-2 positivity was found to be highest among T4 tumors [53.8% (35/65); χ2 = 8.22, P = 0.042] than the lower size tumors. With regard to histological type of breast cancer, ductal carcinoma, which was found to be the most common type (90.4%; 291/322), was found to be more often ErbB-2 positive (46.4%; 135/291), with a χ2 value of 15.42 and P-value of < 0.001. A sub-set of patients (179 cases) for whom follow-up was available was analyzed for disease-free survival and ErbB-2 status. It was found that the patient group that had disease-free survival was less often overexpressing ErbB-2 (36.2%; 47/130) while the other group, which either has recurrence, metastasis or death during the study was more often overexpressing ErbB-2 (75.5%; 37/49), with a χ2 value of 22.13 and a P-value of < 0.001. Surprisingly, both ER and PR status failed to inversely correlate with ErbB-2 overexpression, unlike reported earlier by others. 40.6% (73/180) of ER-positive cases and 48.9% (87/178 cases) of ER-negative cases were found to be ErbB-2 +ve (χ2 = 2.51, P = 0.114). Similarly, 41.7% (70/168) PR-positive cases and 47.4% (90/190) PR-negative cases were found to be ErbB-2 +ve (χ2 = 1.17, P = 0.279). Combined expression of ER and PR also failed to correlate inversely with ErbB-2 status [Table - 1 a] [Table - 1 b]. Survival analysis revealed that ErbB-2 overexpression, positive lymphnode, stage IV disease and the presence of distant metastasis were found to be poor prognostic indicators. At 40 months of follow-up, 83.8% of ErbB-2-negative individuals had disease-free survival whereas only 46.1% of ErbB-2-positive individuals had disease-free survival [Figure - 3]A; χ2 = 25.94, P < 0.001. This suggests an inverse correlation between ErbB-2 status and disease-free survival, as reported earlier. While patients with positive lymphnode had fewer patients (59.5%) with disease-free survival at 40 months during follow-up, the majority of the lymphnode-negative patients (84.0%) had disease-free survival [Figure - 3]B; χ2 = 12.68, P < 0.001. On further analysis, we found interestingly that the group that is positive for both ErbB-2 overexpression and lymphnode had the worst prognosis, with only 41.4% of this group having disease-free survival at 40 months [Figure - 3]E; χ2 = 32.57, P < 0.001. On correlation of stage of the disease with patient survival, we found very interesting results. Stage 1 patients had the best prognosis, with 100% of them being normal with disease-free survival while stage 4 patients had worse prognosis, with 23.3% of them being normal at 40 months of follow-up [Figure - 3]C; χ2 = 28.04, P < 0.001. Stage 2 and 3 patients had better prognosis than stage 4 patients (85.9 and 67.2% respectively). Similar to lymphnode status, presence of distant metastasis was found to be a poor prognostic indicator. Patients with distant metastasis had fewer (22.0%) disease-free survivals at 40 months of follow-up. On the other hand, patients with no metastasis had a larger number (71.6%) of disease-free survivals [Figure - 3]D; χ2 = 19.49, P < 0.001. ER/PR status was not found to influence the prognosis (data not shown). Other factors like age, menopausal status, tumor size and grade were not found to influence the survival pattern (data not shown). Discussion In this study, we analyzed the incidence of ErbB-2 overexpression in Indian sporadic breast cancer patients and correlated the ErbB-2 expression with various clinico-pathological parameters, including patient survival. Various studies have shown 15-30% ErbB-2 positivity by immunohistochemcial staining in sporadic breast cancers worldwide. [6],[17] However, the frequency of ErbB-1/2 overexpression among Indian studies is reportedly higher than that of other reports. Ray et al. reported a 42.0% incidence of ErbB-2 over expression by immunohistochemistry. [18] In another study, Bhatavdekar et al. reported a 68% positivity for ErbB-2. [19] In our study, we found that 43.2% of sporadic breast cases are positive for ErbB-2 overexpression by immunohistochemistry and 25.5% by genomic PCR. Similar discrepancy between genomic amplification and protein levels has been reported. [15] The difference in ErbB-2 positivity between immunohistochemical staining and genomic PCR methods could be attributed to other mechanisms of ErbB-2 overexpression. It has been shown that different transcriptional and post-transcriptional mechanisms are responsible for the increased levels of ErbB-2 transcript and protein. [15] No statistically significant association was obtained between ErbB-2 overexpression and the following parameters: patient age and menopausal status, tumor grade, stage of disease and distant metastasis. Literature reports an inverse relationship between ErbB-2 and steroid receptors (ER and PR). [12],[13],[14] While a similar inverse correlation was not apparent in our study, we found that approximately 59.4% of ER-positive and 58.3% PR-positive tumors were ErbB-2 negative. However, this data was not statistically significant (χ2 = 2.51, P = 0.114; χ2 = 1.17, P = 0.279 respectively). A positive correlation between lymphnodes and ErbB-2 overexpression has been reported. [20],[21] However, some studies found no association between lymphnode status and ErbB-2 expression levels. [22] In our study, lymphnode status was positively associated with ErbB-2 status. Our study also showed that larger-sized tumors had more overexpression of ErbB-2 compared with smaller-sized tumors, with T4 tumors having higher expression of ErbB-2, which is consistent with other published reports. [23] Further, we found that ErbB-2 overexpression was also more in ductal carcinoma of the breast compared with lobular and other types. This is also consistent with the reported literature, where more ErbB-2 overexpression is described in ductal carcinoma of the breast. [24] ErbB-2 overexpression either alone or along with other clinical parameters has been shown to be associated with poor prognosis in many studies. [25],[26],[27],[28] Our results show that ErbB-2 overexpression is a marker for poor prognosis. Further, patients with ErbB-2 overexpression along with positive lymphnode had worse prognosis. In addition to ErbB-2 status, positive lymph node, stage IV disease condition and presence of distant metastasis were all found to be poor prognostic indicators. [29] However, other parameters like tumor size, grade, age and menopausal status were all found to have no effect on survival pattern consistent with published reports. [25],[26],[27],[28] Thus, our data clearly demonstrates prognostic significance as well as its association with other parameters like lymphnode status, tumor size and ductal carcinoma, thereby emphasizing the importance of ErbB-2 status determination on breast cancer treatment programme. Acknowledgments KS is a Wellcome Trust International Senior Research Fellow. KV is supported by a DBT post-doctoral fellowship. Infrastructural support by funding from ICMR (Center for Advanced studies in Molecular Medicine), DBT (Program support and Genomics program), DST (FIST) and UGC (Special assistance) is acknowledged.[33] References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10004t1b.jpg] [cn10004f1.jpg] [cn10004t1a.jpg] [cn10004f2.jpg] [cn10004f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}