 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
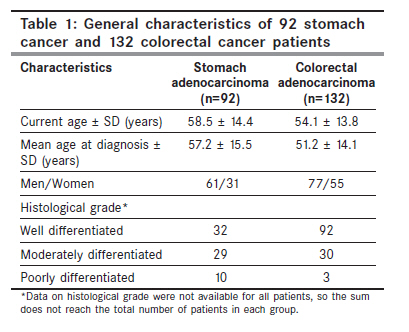
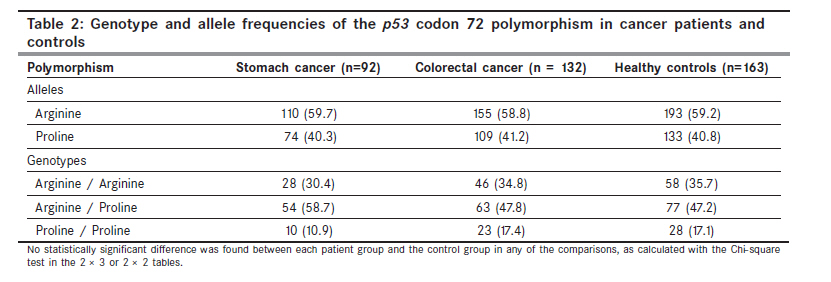
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 31-34 Original Article p 53 codon 72 polymorphism in stomach and colorectal adenocarcinomas in Iranian patients Mojtahedi Z, Haghshenas MR, Hosseini SV1, Fattahi MJ, Ghaderi A Shiraz Institute for Cancer Research, Shiraz University of Medical Sciences, Shiraz, Iran, 1 Gastroenterohepatology Research Center, Namazee Hospital, Shiraz, Iran Code Number: cn10008 PMID: 20071787 DOI: 10.4103/0019-509X.58856 Abstract Background: The association of a functional single nucleotide polymorphism at codon 72 of the p53 gene (Arg72Pro) with malignancy is a subject of controversy. We analyzed this polymorphism in 224 patients with gastrointestinal cancers (92 with stomach cancer and 132 with colorectal cancer) and in 163 healthy controls. Material and Methods: DNA was extracted from peripheral blood mononuclear cells and amplified with an allele-specific polymerase chain reaction. Results: There was no significant association between p53 alleles and gastrointestinal cancers. The frequency of the Arg allele was 59.7, 58.8, and 59.2% in the stomach cancer patients, colorectal cancer patients, and controls, respectively. Frequencies of the Pro allele were 40.3% in patients with stomach cancer, 41.2% in patients with colorectal cancer, and 40.8% in controls. Likewise, genotype frequencies did not differ significantly between the two patient groups and controls. There were no differences in genotype or allele frequencies by gender, age, or histological grade. Conclusions: The data do not support the association of the p53 codon 72 polymorphism with stomach or colorectal cancers in Iranian patients.Keywords: Colorectal cancer, polymorphism, p53, stomach cancer Introduction The tumor suppressor and transcription factor p53, first described in 1979, [1] is a critical modulator of the cellular response to various stresses. Downstream events mediated by p53 can promote (1) transient cell cycle arrest to allow for DNA repair, and (2) programmed cell death, to remove the irreparably injured cells. Normally p53 is present only in minute amounts in the cell because of its short half-life. Upon cellular stress, p53 is modified and exerts a sequence-specific DNA binding activity. [2] This tumor suppressor is one of the most frequently studied molecules in malignant processes. [2] Stomach cancer is the fourth most frequent cause of cancer worldwide, with 930 000 cases diagnosed in 2002 (8.6% of all new cases). [3] The disease is much more frequent in Iran, and ranks as the most common form of cancer, with 7900 new cases (15.5% of all new cases) in 2002. [4] Colorectal cancer is the third most common cancer throughout the world, and accounts for about 1 million new cases each year (9.4% of the world total). [3] In Iran, it ranks fourth in frequency, and there are approximately 3700 new cases of colorectal cancer yearly. [4] In terms of mortality, stomach cancer is the second-most lethal cancer worldwide (700 000 deaths per year) after lung cancer, [3] and is the top cancer-killer (6700 deaths per year) in Iran. [4] Colorectal cancer is the fourth-ranked cancer-killer in the world (about 529 000 deaths per year) [3] and accounts for about 2300 deaths per year in Iran. [4] The p53 gene, located on chromosome band 17p13.1, is susceptible to somatic mutation, and up to 50% of the patients with gastrointestinal (GI) cancers were reported to have such p53 alterations. [2] Mutant proteins are defective in DNA binding in a sequence-specific manner, and thus in the upregulation of downstream genes. [2] Despite the strong association of somatic p53 gene mutations with malignant processes, [2] the association of germline polymorphisms of p53 with malignancies is the subject of controversy in different ethnic backgrounds and in different types of cancer. [5],[6],[7],[8],[9],[10],[11],[12],[13],[14] At least 13 polymorphisms have been described in this gene. [14] The most commonly studied one is a single nucleotide polymorphism (SNP) at codon 72 in exon 4 of the p53 gene, which results in the substitution of arginine (Arg) by proline (Pro) in the transactivating domain. [14] These polymorphic variants alter the structure and function of the p53 protein. [15] The potential consequences of this amino acid exchange are differences in the susceptibility to malignant transformation, induction of apoptosis, and transcriptional activity. [16] , The p53 codon 72 Arg/Pro polymorphism is reportedly a genetic risk factor for stomach or colorectal cancer. [6],[7],[8],[13] However, other reports have failed to confirm this association. [5],[9],[10],[11] The discrepancies between studies may be related in part to significant differences in the genotype distribution of the p53 codon 72 among ethnic groups. [17] The role of this SNP in stomach and colorectal cancers has apparently not been investigated in Iran. The aim of the present study is to determine the frequency of the p53 gene codon 72 polymorphism in a sample of Iranian patients with stomach or colorectal cancer. Materials and Methods Subjects All participants were informed that blood samples would be used for genotyping, and their consent was obtained. The study was approved by the Ethics Committee of the Shiraz University of Medical Sciences. The patients were 92 unrelated individuals with stomach cancer (61 men and 31 women; mean age 58.5 ± 1 4.4 years) and 132 with colorectal cancer (77 men and 55 women; mean age 54.1 ± 13.8 years). From the patients' medical records we obtained data on the gender, age, and histological grade [Table - 1]. Histologically, adenocarcinoma was confirmed in all patients. Control individuals were 163 unrelated healthy volunteers (93 men and 70 women; mean age 58.2 ± 13.1 years) residing in the same region as the patients. Control participants did not have any type of cancer or first-degree family history of cancer. DNA preparation and polymerase chain reaction Genomic DNA was extracted from lymphocytes with a salting-out method. [18] Genomic DNA was amplified by the allele-specific polymerase chain reaction (PCR), as described previously. [19] The PCR amplification produced a 177-bp fragment for the Pro allele and a 141-bp fragment for the Arg allele. Statistical analysis Genotype frequencies were tested for the Hardy-Weinberg equilibrium, and chi-squared tests were used to test the fit to the equilibrium. The data were analyzed with SPSS v. 11.5.0 software (SPSS, Chicago, IL, USA). The difference in age at the onset, according to the p53 codon 72 polymorphism, was calculated with one-way analysis of variance (ANOVA). Differences in gender and histological grade according to the polymorphism were sought with Pearson's chi-square test or Fisher's exact probability test, as appropriate. Differences were deemed statistically significant at a P value less than 0.05. Odds ratios (OR) and their 95% confidence intervals (CI), computed from binary logistic regression analyses with adjustment for age and sex, were used to estimate the association between the p53 codon 72 polymorphism and the histological grade. Results The frequencies of genotypes in the patient and control groups were in agreement with the Hardy-Weinberg equilibrium (data not shown). The p53 codon 72 polymorphism (CGC-arginine or CCC-proline) was determined in 224 patients with GI cancer and in 163 healthy controls [Table - 2]. Of 224 patients, 92 had stomach adenocarcinoma and 132 had colorectal adenocarcinoma (107 in the colon and 25 in the rectum). There was no significant association between the genotypes and GI cancers (P = 0.17 in stomach cancer, P = 0.99 in colorectal cancer). Likewise, allele frequencies in the two patient group did not differ significantly from those in the controls (P = 0.89 in stomach cancer, P = 0.90 in colorectal cancer). The frequency of the p53 codon 72 polymorphism was also compared between genders, and was similar in men and women (P 0≥ 0.05). Among the 61 men with stomach cancer, 20 (32.7%), 37 (60.7%), and 4 (6.6%) had the Arg/Arg, Arg/Pro, and Pro/Pro genotypes, respectively. Among the 31 women with this diagnosis, these frequencies were 8 (25.8%), 17 (54.9%), and 6 (19.3%), respectively. The Arg allele frequency was 77 (63.1%) in male patients and 33 (53.2%) in female patients. The Pro allele frequency was 45 (36.9%), and 29 (46.8%) in male and female patients, respectively. In colorectal cancer, the frequencies of Arg/Arg, Arg/Pro, and Pro/Pro genotypes were 28 (36.4%), 36 (46.7%), and 13 (16.9%) in 77 men, and 18 (32.8%), 27 (49.0%), and 10 (18.2%) in 55 women. The frequencies of Arg and Pro alleles were 92 (59.7%) and 62 (40.3%) in men, and 63 (57.3%) and 47 (42.7%) in women. The mean age of onset of stomach or colorectal cancer did not differ among patients according to the p53 72 genotype or allele (P ≥ 0.05). Data on the histological grade were available for 71 of 92 stomach cancer patients and 125 of 132 colorectal cancer patients [Table - 1]. No association was found between the p53 codon 72 polymorphism and the histological grade (data not shown). After adjustment for age and sex, the association between the histological grade and the polymorphism remained nonsignificant. When compared with Arg/Arg homozygotes, the adjusted ORs in the Pro allele carriers for having grade I vs. Grade II/III disease were 0.34 (95% CI .08 1.43) in stomach cancer, and 0.69 (95% CI 0.18 - 2.57) in colorectal cancer. Discussion In Iran, stomach cancer accounts for 15% of malignant tumors, and colorectal cancer accounts for approximately 8% of all malignancies. [4] Both cancers vary widely in geographical distribution. Colorectal cancer is more prevalent in western countries, whereas, stomach cancer has a very high incidence in some Asian countries, including Iran. [4] Although each disease has a unique etiopathogenesis, they share some risk factors such as diet (low intake of fruits and vegetables) and aging. [20] As the p53 tumor suppressor gene is involved in DNA repair, cell cycle, gene transcription, and apoptosis, it represents a potential genetic risk factor for the development or progression of cancer. [2] The p53 codon 72 Arg/Pro polymorphism has been linked to cancer susceptibility in a variety of malignant processes, notably lung cancer, however, these findings remain controversial. [3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[19] This controversy might be due to the fact that the genotype distribution of the p53 codon 72 Arg/Pro polymorphism differs significantly with race. [19] For instance, Shepherd et al. showed that Arg/Arg genotype frequency was 64% in whites as compared to 24% in blacks. [19] Moreover, the activity of this SNP might vary depending on the type of the cancer. Langerod et al. investigated correlations between the codon 72 polymorphism and somatic p53 mutations in breast cancer and colorectal cancer cells, and reported that the p53 codon 72 polymorphism may influence the function of p53 mutations in breast carcinoma, but not in colorectal carcinoma. [21] More than 90% of stomach and colorectal cancers arise from adenocarcinoma. [20] We investigated the allele and genotype frequencies of the p53 codon 72 Arg/Pro polymorphism in stomach and colorectal adenocarcinoma patients and compared them to those in healthy individuals from the population of southern Iran. In agreement with prior studies on breast cancer in Iran, [19] we found nonsignificant differences in the genotype or allele frequencies between the patients and the control groups. Moreover, we found no significant association, between p53 alleles and genotypes with regard to gender, age, or histological grade. A number of studies have failed to demonstrate the association between the p53 codon 72 polymorphism and stomach or colorectal cancers. [5],[9],[10],[11] For example, Hamajima et al. analyzed this SNP in 144 stomach cancer patients, 147 colorectal cancer patients, and 241 non-cancer patients, in a Japanese population, and found no significant association between the genotype or allele frequencies and the diseases. [5] However, other studies found the p53 codon 72 polymorphism to be a genetic risk factor for stomach or colorectal cancers. [7] For example, Mammano et al. examined the p53 codon 72 polymorphism in 90 patients with colorectal cancer and 321 age-matched controls and 322 centenarians, and observed that the Arg allele was significantly more frequent in patients than in age-matched controls and centenarians. [7] Other researchers did not find a significant association between this SNP and stomach or colorectal cancer patients as a whole, but categorizing the patients according to sex, age, or histological grade, revealed significant differences in genotypes according to these parameters. [6],[7],[8] For instance, the study of Jones et al. concluded that Arg/Pro heterozygotes developed colorectal cancer 13 years earlier than Arg/Arg homozygotes. [8] However, the p53 codon 72 polymorphism did not modify the age onset of the disease, sex, or histological grade in other ethnic backgrounds. [9],[11],[13] There are further stratified studies in which the genotype distribution was associated with other clinicopathological parameters such as tumor location, distant metastasis, or survival. [7],[13] These parameters are not assessed here. In conclusion, the present study shows that the p53 codon 72 polymorphism is not associated with an overall increased risk of stomach and colorectal cancers in Iranian patients. Also gender, age, and histological grade are not influenced by this SNP. Further studies, with larger numbers of patients, are required to examine the possible contribution of other clinicopathological parameters of the diseases with the p53 codon 72 polymorphism. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10008t1.jpg] [cn10008t2.jpg] |
| |||||||||


{kind=link}
{kind=link}