 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
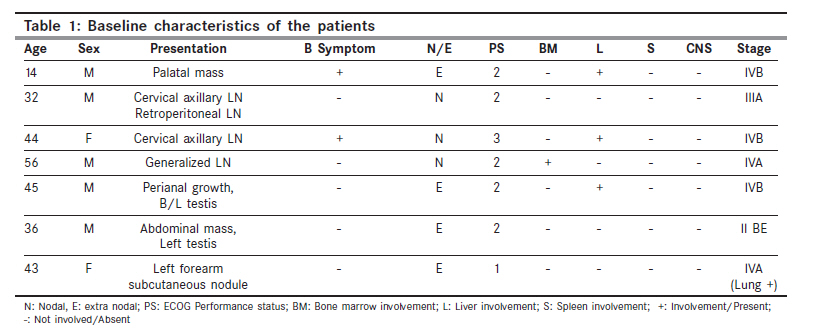
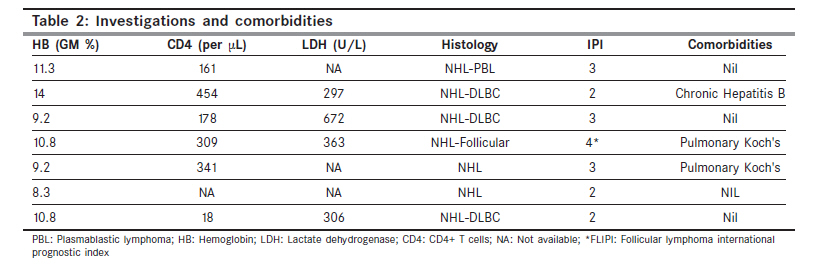
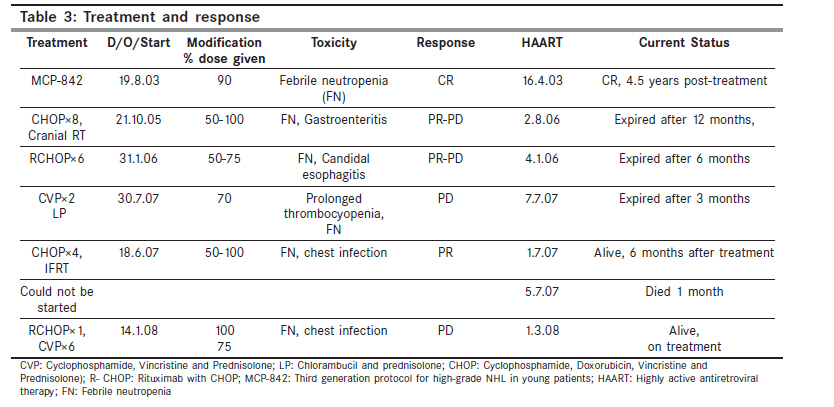
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 35-39 Original Article HIV-associated non-Hodgkin's lymphoma: Experience from a regional cancer center Sharma A, Bajpai J, Raina V, Mohanti BK1 Departments of Medical Oncology, 1 Radiation Oncology, Dr BRA IRCH, AIIMS, New Delhi, India Code Number: cn10009 PMID: 20071788 DOI: 10.4103/0019-509X.58857 Abstract Aims : To analyze clinical features and survival in HIV-associated non-Hodgkin lymphoma (NHL) cases registered at Dr BRA Institute Rotary Cancer Hospital of AIIMS, New Delhi. Materials and Methods : We have retrospectively reviewed records of NHL patients registered, from January 2003 to July 2007 to analyze HIV-associated NHL. Results : Seven cases of HIV-associated NHL cases were identified. Age range was 14-56 years. Five were males. Baseline performance status (ECOG-PS) was >I in 6. Mean LDH was 409 U/L. Mean hemoglobin was 10.5 g% and mean CD4 count was 243/mm3 (range 18- 454). Three cases had nodal lymphoma and four had extra nodal lymphoma. No primary CNS (PCNSL) lymphoma was seen. All patients were of advanced stages and of intermediate to high-risk group based on international prognostic index (IPI). Six cases had high-grade NHL. None had CNS involvement. Five had B symptoms. HIV infection was diagnosed as part of NHL work-up in five patients. All patients received HAART. All were planned for chemotherapy with CNS prophylaxis. Protocols used were CVP, CHOP, R-CHOP or MCP-842. One patient received IFRT. Response : One patient achieved complete response (CR) and continues to be disease free, with 4.5 years of follow-up. Three cases achieved partial response (PR) and 2 had progressive disease (PD). Currently, three patients are on follow-up. Conclusions : These NHL are of higher grade and advanced stage. Response and tolerance to chemotherapy is poor. Appropriate supportive care and CNS prophylaxis might improve outcome. We need to improve epidemiological data collection system in this part of world. With HAART, the goal of therapy is durable CR rather than palliation.Keywords: Acquired immune deficiency syndrome, human immunodeficiency virus, non-Hodgkin lymphoma Introduction While incidence rates of NHL (non-Hodgkin lymphoma) in India are lower than Australia and Western countries such as Canada and United States (10-17 per 100,000 populations), NHL is one of the common cancers in urban populations in India. Among the urban population-based cancer registries (PBCRs) in India, Delhi has the highest rates of 5.1 per 100,000 persons per year. This is followed by Mumbai, Chennai, Bhopal and Bangalore, in the decreasing order. [1] NHL occurs at greatly increased rates in people with HIV compared with the general population and generally has a poor prognosis. [2],[3] The introduction of highly active antiretroviral therapy (HAART) in the mid-1990s has led to marked declines in the incidence of most AIDS-associated illnesses, but the incidence of AIDS-associated NHL (ARL) has declined less. [4],[5],[6],[7] ARL is now the second most common AIDS-associated malignancy, and is the AIDS-defining diagnosis in approximately 3% of HIV-positive patients, although it is uncertain what percentage of patients already diagnosed with AIDS develop lymphoma. In Australia, the proportion of AIDS cases presenting as NHL has increased from 4.4% (before the introduction of HAART) to 6.3% after 1996. [8] Similar findings have also been reported from the United States and Europe. [9],[10] HIV prevalence in India is approximately 0.36% in the age group of 15-49 years, accounting for 2-3.1 million people. [11],[12] Historically, patients with NHL and AIDS have been more likely to present with extranodal NHL and high-grade histological findings. [13] They have been less likely to respond to chemotherapy, with shorter overall survival. Reported predictors of poor survival included low CD4 count at diagnosis, having a prior ADI (AIDS defining illness), CNS presentation, other extranodal presentation, advanced stage of NHL, high LDH levels and older age. [3],[14] Most of these variables reflect advanced NHL/HIV. While some studies have demonstrated an improved survival in HIV-associated NHL since the use of HAART, [15],[16],[17],[18],[19] others have found no substantial changes in survival. [7],[20],[21],[22] In light of these conflicting findings, this case series analyses clinical features and survival of HIV-associated NHL patients. This series may not reflect the true numbers of HIV-associated NHL seen in All India Institute of Medical Sciences as some cases are being treated in other departments. Materials and Methods We have retrospectively reviewed records of NHL patients examined by us from January 2003 to July 2007 to identify and analyze survival of HIV-associated lymphoma. HIV infection was diagnosed as part of routine NHL work up in 5 patients and only 2 had report of HIV upfront. Information about histology, LDH, CD4 counts, stage and outcome was collected. Results [Table - 1] shows the baseline patients characteristics. Age range was 14-56 years, and 2 patients were female. Six of the patients presented with advanced stage (stage III/IV). All except one had ECOG PS of two or more. Investigation profile is shown in [Table - 2]. Hemoglobin was in the range of 8.3-11.3 gm/dl (mean 10.5) . Baseline CD4 count was in the range of 18-454/mm 3 with a mean value of 243/mm 3 . All were of intermediate to high-risk group based on IPI. WHO classification was used for typing of NHL. Six cases had high grade histology. None had CNS involvement. Five had B symptoms. Three patients also had extranodal involvement. All patients were planned for chemotherapy with CNS prophylaxis (6 received intrathecal chemotherapy, 1 received cranial RT). Chemotherapy doses were modified due to poor tolerance. Decisions about treatment protocol chosen were based on histology, PS, stage, affordability and prevailing practice at that point of time. Overall response was poor. One patient achieved CR and is still in remission till the last follow-up. Two achieved PR but one progressed later on. Two had progressive disease. Four of seven patients succumbed to illness. Two died after completion of treatment, one on treatment and one before receiving any treatment. Three patients are under follow-up (one disease free). Comorbidities were Koch's in two (received anti-Koch's treatment), and chronic hepatitis B in one. In [Table - 3], treatment given and response to treatment is shown. Discussion HIV prevalence in India reflects that it is one of the countries with the highest HIV burden. In the developed countries, 34% of AIDS patients suffer from cancer, while this incidence is only 3%-4% in the Indian population. [23] Even though, NHL occurs at greatly increased rates in people with HIV compared to the general population there is sparse data available on HIV-associated NHL from this region, possibly due to underdiagnosis and inadequate reporting system. Lymphoma in this population is likely to be of advanced stage, higher grades and poor responsiveness to therapy. Overall tolerance to aggressive treatment is poor, requiring frequent dose modifications, delaying of treatment and incomplete treatment. Inappropriate treatment and inability to maintain dose density and intensity in the background of aggressive disease are determinants of poor response to therapy. As reflected in this series, in five of seven patients, HIV was reported as part of NHL workup and only 2 patients had history of HIV infection before being diagnosed as NHL. Another reason for low incidence could be early death in these patients on account of opportunistic infections and inadequate treatment. HIV-positive patients from many parts of the country did not have the proper access to HAART because of economic constraints or lack of health facility in nearby location. However, now through the NACO (National AIDS Control Organization), HAART is available free of cost since April 2004. This scheme was launched initially at 8 institutions is now available in 31 states and Union Territories at 163 centers. Several other studies analyzed clinical features, prognostic factors, response to treatment and survival statistics in HIV-associated NHL patients. Diamond et al[24] used the San Diego/Orange County cancer registry to identify 64 cases of NHL with AIDS who received HAART at the time of NHL diagnosis or thereafter and 64 matched NHL controls without AIDS. Thirty-three percent of HIV cases had high-grade histology versus 11% of controls (P < 0.01); overall median survival was 16 months for cases versus 99 months for controls (P < 0.01). Among 40 matched pairs of cases and controls who received chemotherapy, 32% of cases received reduced-dose chemotherapy versus 5% of controls (P < 0.01) and median survival was 33 months for cases and 99 months for controls (P < 0.44). Author concluded that patients with AIDS-related NHL who received HAART had high-grade histology and baseline cytopenias and received reduced-dose chemotherapy more often than patients without AIDS. However, AIDS patients who received HAART and chemotherapy had survival similar to NHL patients without AIDS, an improvement from the pre-HAART era. Chow et al[25] retrospectively analyzed 257 cases of AIDS-related NHL (among 2004 patients with HIV infection) treated at the University Hospital of Frankfurt, Germany, from January 1983 to May 1999. Patients received CHOP-like therapy as standard treatment and found that during study period incidence of NHL was decreasing (1991-1994: 14.2% versus 1995-5/99: 12.8%). Decrease was mainly in the low-grade NHL and PCNSL, whereas the incidence of high-grade B cell NHL increased compared with all diagnosed cases of NHL (1983-1986: 53.3% versus 1995-5/99: 78.6%). One-year survival probability of all screened patients with AIDS-related NHL was 54%, while 5-year survival rate remained 5%. Age < 25 years, development of NHL in the years before 1990, intravenous drug users (IVDU), CD4 counts < 150/mm 3 , PCNSL as well as NHL as the AIDS index disease, were significant independent predictors of poor survival. Overall survival of patients was prolonged with HAART. Data from Sydney hospitals (1985-2001) were published by Robotin et al. [26] Statistical comparisons were made between the pre-HAART and post-HAART era. Three hundred cases of AIDS-related NHL were identified. Forty-three percent of their patients had stage III or IV compared with 85% of ours. Fifty-eight percent patients in their series had NHL as AIDS defining illness compared with 71% in the series reported here. Divergent trends were identified for systemic and primary CNS NHL. More patients in post-HAART era presented with NHL as first AIDS defining illness whether systemic or primary CNS, higher CD4 counts (median 208 compared with 114 in pre-HAART era), early-stage disease. Median survival time increased from 4.2 months in 1985-1991 to 19 months in the post-HAART era (P < 0.001). In multivariate analysis, predictors of poor survival for systemic NHL included NHL diagnosis after another AIDS-defining illness, stage 4 NHL, presentation at extralymphatic sites, and nonreceipt of chemotherapy. After adjusting for the factors, those diagnosed in the era of HAART had a significant 56% reduction in the rate of death (P < 0.001). In this case series, we have seen that HIV-associated NHL occurs at comparatively younger age (mean 37.83 years) compared with median of 39 and 44 years as reported by others. [24],[25] Male preponderance seen here has also been reported earlier by Diamond [24] and Chow. [25] We have seen male to female ratio of 5:2 compared with 10:1 by Diamond et al[24] and 49:1 by Chow et al. [25] This may be reflection of higher incidence of HIV positivity in male population. All patients received HAART so its association with response and outcome could not be studied. Similarly, CD4 count was> 150/µl in all except one at presentation, so association of low CD4 counts with the results could not be verified. Wolf et al[27] in a retrospective analysis of 214 cases of AIDS-related lymphoma treated from January 1984 until May 2003 showed that prolonged survival was significantly associated with the achievement of a complete remission and a favorable virological response to HAART. In a study conducted at the Tata Memorial Hospital (TMH), Mumbai, among HIV-positive cancer cases during the period 2001-2005, increased proportion of NHL was observed. Proportionate incidence ratio (PIRs) in males was 17.1, 95% CI 13.33-21.84, and 10.3 in females, 95% CI 6.10-17.41). The absence of Kaposi sarcoma and increased PIRs for certain non-AIDS-defining cancers among HIV-infected cancer cases indicate a different spectrum of HIV-associated malignancies in this region. [28] Conclusions Our case series has limitations of small sample size and short follow-up duration; however, we could still derive the conclusion that HIV-associated NHL are of higher grade and advanced stage. Tolerance to chemotherapy is generally poor and dose modifications in the background of aggressive disease are one of the determinants of poor response to therapy. Careful attention should be paid to central nervous system chemoprophylaxis, opportunistic infection prophylaxis and potential drug interactions between cytotoxic and antiretroviral therapies. We believe that there is an urgent need to improve collection of epidemiological data and to direct research efforts to explain a strikingly low incidence of cancer in Indian subjects compared with that in the West. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10009t3.jpg] [cn10009t2.jpg] [cn10009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}