 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
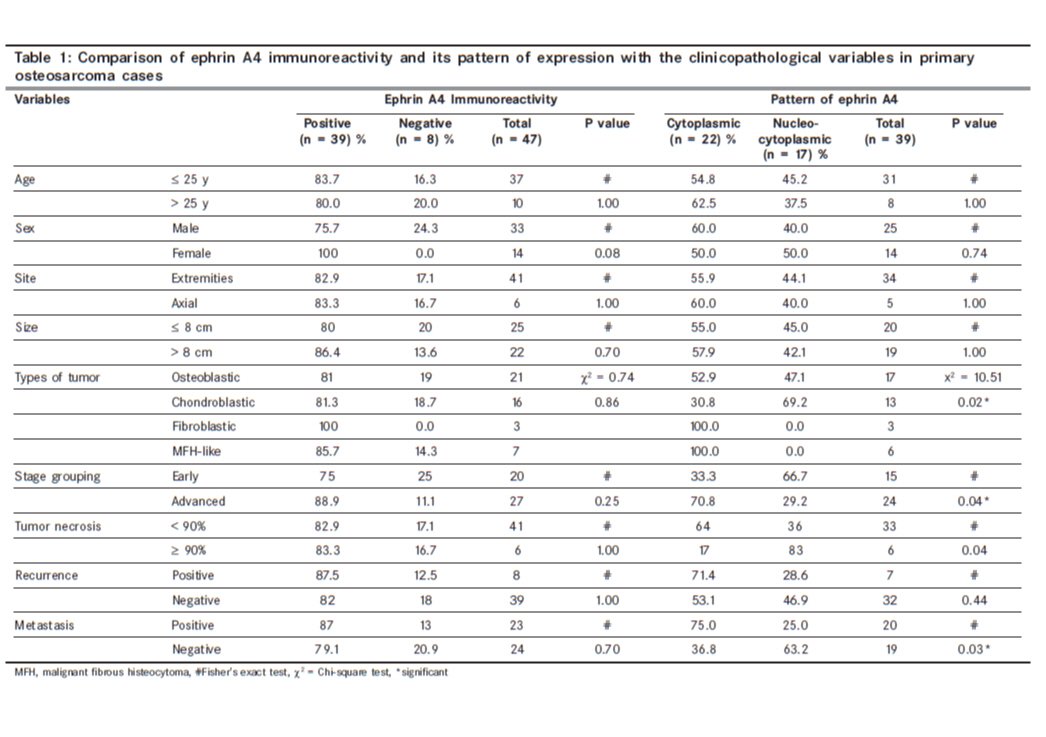
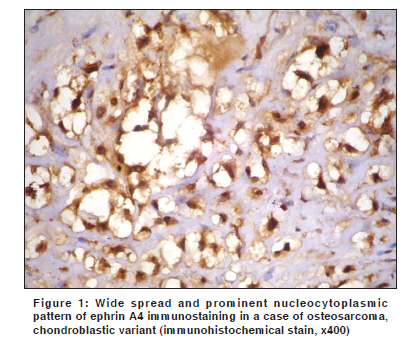
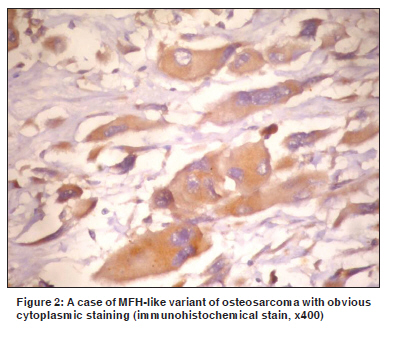
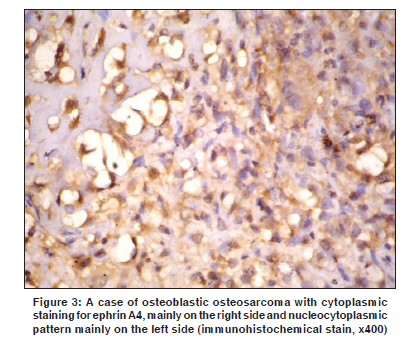
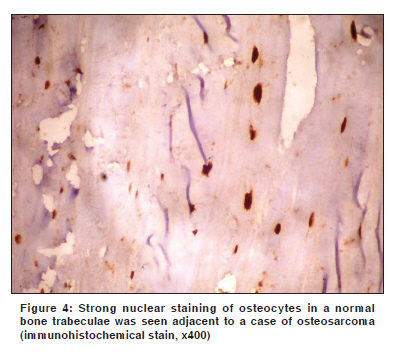
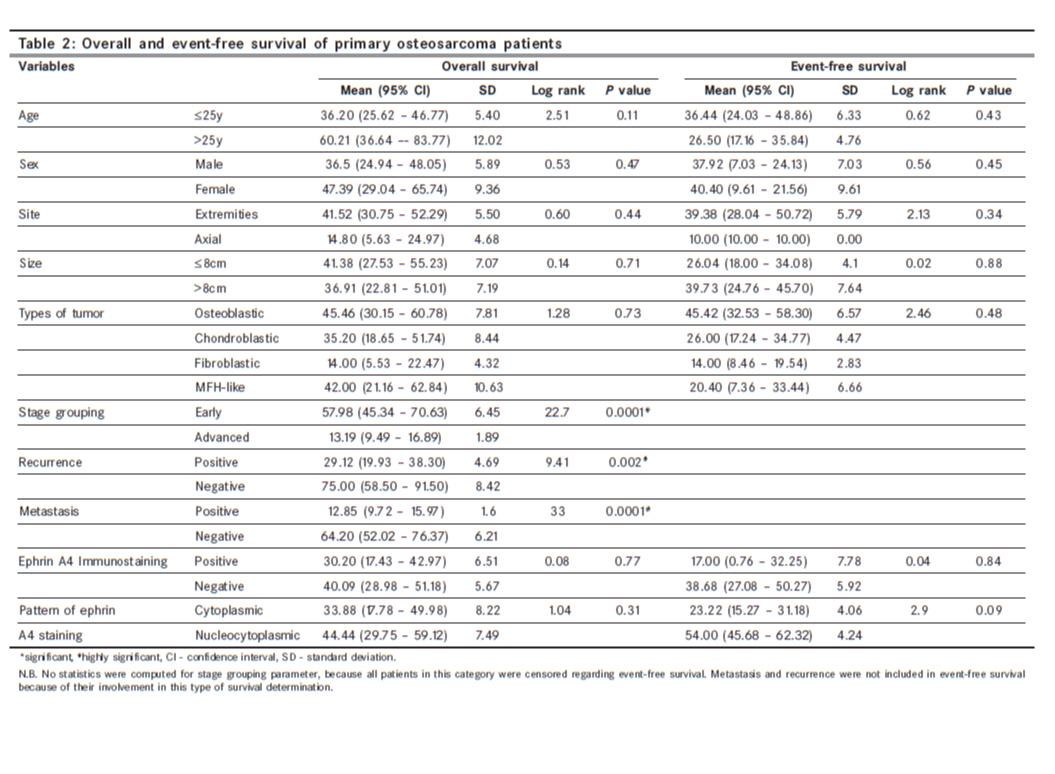
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 46-52 Original Article Ephrin A4 expression in osteosarcoma, impact on prognosis, and patient outcome Abdou AG, Abd El-Wahed MM, Asaad NY, Samaka RM, Abdallaha R Department of Pathology, Faculty of Medicine, Menofiya University, Shebein Elkom, Egypt Code Number: cn10011 PMID: 20071790 DOI: 10.4103/0019-509X.58859 Abstract Background : Ephrin A4 is one of the ephrin ligand molecules belonging to the tyrosine kinases receptor family. It was originally identified in a T-lymphoma cell line and seen to be expressed in human adult tissue as well as several tumor types. In our previous study, we showed the unique pattern of ephrin A4 immunohistochemical staining, which differed according to the type of examined bone specimens (normal bone, primary, and metastatic osteosarcoma lesions). The aim of the present study is to evaluate the prognostic impact of ephrin A4 expression in a group of primary osteosarcoma patients. Materials and Methods : Ephrin A4 immunohistochemical expression was carried out on 47 primary osteosarcoma cases. Results : Ephrin A4 was expressed in 82.9% of osteosarcoma cases with cytoplasmic localization in 58.9% of positive cases. The cytoplasmic pattern was significantly associated with aggressive histopathological types of osteosarcoma (P = 0.02), advanced stage (P = 0.04), the presence of metastasis (P = 0.03), inferior response to neoadjuvent chemotherapy (P = 0.04), and tended to be associated with a shorter event-free survival (P = 0.09). Conclusions : The cytoplasmic pattern of ephrin A4 could identify a subgroup of primary osteosarcoma patients with a high liability for progression, poor prognosis, and inferior response to chemotherapy.Keywords: Ephrin A4; osteosarcoma; prognosis; response to chemotherapy Introduction Osteosarcoma is the most common primary malignant bone tumor following myeloma and lymphoma. [1] In Egypt, osteosarcoma is twice more common than chondrosarcoma and three times more frequent than Ewing's sarcoma. [2] It accounts for approximately 29% of primary bone tumors according to El-Bolkainy et al. 2005 [2] and 47.75% according to the last registry of the Egyptian National Cancer Institute. [3] Receptor tyrosine kinases comprise 14 distinct members, the largest of which is the Eph family. The family is divided by sequence identity into two classes, EphA and EphB, with corresponding transmembrane ligand families, called type A and type B ephrins. Ligand-receptor binding results in forward and reverse signaling which have been implicated in a range of physiological functions. [4] Ephrin A4, one of ephrin ligand molecules, was originally identified in a T-lymphoma cell line and seen to be expressed in human adult tissues such as spleen, prostate, ovary, small intestine, and colon. [5] Ephrin A4 is also upregulated in several tumor types such as leukemia and lymphoma. [6] In our previous study, we showed the unique pattern of ephrin A4 expression in different bone specimens. [7] In that study, we demonstrated the presence of cytoplasmic and nucleocytoplasmic staining patterns for ephrin A4 immunoreactivity. The cytoplasmic pattern was the only pattern seen in metastatic osteosarcoma lesions and the nucleocytoplasmic pattern was seen in all normal bone specimens. [7] The two patterns were seen in primary osteosarcoma cases with a different percentage of positivity. [7] This apparent difference in the distribution of ephrin A4 pattern of staining requires further correlation with the tumor histopathological characteristics as well as its impact on patient outcome. The aim of the present study is to evaluate the prognostic impact of ephrin A4 expression in a group of primary osteosarcoma patients. Materials and Methods This study investigated 47 primary osteosarcoma cases obtained from the Pathology Department, Faculty of Medicine, Menofiya University, between January, 2000 and January, 2007. The primary diagnostic specimens were evaluated for ephrin A4 expression, while the postoperative resection specimens were reviewed to assess the extent of necrosis. The percentage of necrosis was further subdivided into < 90% and ≥ 90%, according to Bacci et al. 2006. [8] Staging of the tumor was performed according to the TNM staging system, [9] in which osteosarcoma is divided into four stage groups termed I, II, III, and IV. Stages I and II were lumped and designated as an early stage, while stages III and IV were lumped and designated as an advanced stage. The preoperative chemotherapy regimen was similar to that described in our previous report. [7] Overall survival: Survival time was calculated in months from the date of diagnosis and ended with the death or the last follow-up visit of the patient. Follow-up data were available for only 43 primary osteosarcoma cases and extended to the end of October 2007. Event-free survival: The event-free interval was calculated in months from the date of treatment (either operative or preoperative chemotherapy) and ended with the date of metastasis or recurrence, whatever the first event was. Data about event-free survival were available for all studied primary osteosarcoma cases (47 cases). Five-micron thick sections prepared from paraffin-embedded blocks were subjected to deparaffinization in xylene, rehydration in a graded series of alcohol, and antigen retrieval, by boiling in 10 mM citrate buffer (pH 6.0) for 20 minutes. The slides were then incubated overnight at room temperature, with ephrin A4 antibody (rabbit polyclonal antibody) (dilution 1:100) (Labvision, California, USA), which was the same antibody used in our previous study. [7] The second antibody used for detection of ephrin A4 binding was Envision+ (DakoCytomation, Glostrup, Denmark). DAB (Diaminobenzidine) and Mayer's hematoxylin were applied as a substrate / chromogen and a counter stain, respectively. Normal brain tissue was used as a positive control, while negative controls were prepared by substitution of a primary antibody with a blocking buffer. Ten percent was considered as the cutoff point for assigning positive staining for ephrin A4 either cytoplasmic or nuclear. [4],[7] In positive cases with mixed staining patterns, the nucleocytoplasmic pattern was assigned as long as the nuclear portion exceeded 10%, otherwise, the cases were designated as having cytoplasmic pattern. [7] Data were collected, tabulated, and statistically analyzed using a personal computer with the "Statistical Package for the Social Sciences (SPSS) version 11" program. Fisher's exact, Chi square, and Mann-Whitney (U) tests were applied in comparison, while the Log rank test was used in the assessment of overall and event-free survival. Cox regression analysis was applied in multivariate survival analysis. Differences were considered statistically significant (S) when p < 0.05 and highly significant (HS) when p< 0.001. Results Ephrin A4 was expressed in 82.9% of the osteosarcoma cases and failed to show any correlation with the studied clinicopathological parameters. However, it tended to be expressed in females more than males (P = 0.08) [Table - 1] (data not shown). The cytoplasmic localization of ephrin A4 was seen in 58.9% of the positive cases and was significantly associated with the histopathological type of osteosarcoma (P = 0.02), stage (P = 0.04), and metastasis (P = 0.03). Ephrin A4 showed cytoplasmic expression in 100% of the fibroblastic and 100% of the malignant fibrous histeocytoma-like (MFH-like) subtypes in comparison to 52.9% in osteoblastic and 30.8% in chondroblastic variants [Figure - 1],[Figure - 2],[Figure - 3],[Figure - 4]. The advancement of stage was statistically associated with a higher percentage of the cytoplasmic pattern, since 70.8% of the cases with an advanced stage showed a cytoplasmic pattern when compared to 33.3% of the cases with an early stage. Furthermore, 15 / 20 (75%) of the positive metastatic cases were of the cytoplasmic staining pattern [Table - 1]. In addition, 95% of the cases with the cytoplasmic pattern of ephrin A4 expression showed a significant association with a lower percentage of necrosis (< 90%) (inferior response to therapy) (Fisher exact test = 0.04). In our study, factors that affected the overall survival and predicted the patient outcome were stage (P = 0.0001), the presence of recurrence (P = 0.002), and metastasis (P = 0.0001). In other words, in patients who presented with an advanced tumor stage, developed recurrence or metastasis were associated with poorer survival than in those who presented with an early stage or lacked recurrence or metastasis [Table - 2]. The development of metastasis was the only independent prognostic factor that affected the patients' survival using Cox regression analysis (odds ratio (OR) = 12.53, P = 0.02). The cytoplasmic pattern of ephrin A4 expression tended to be associated with shorter, event-free survival in comparison to the nucleocytoplasmic one, although this tendency lacked significance (P = 0.09) [Table - 2]. Discussion The present study confirms our earlier observation that ephrin A4 has two patterns of staining, cytoplasmic and nucleocytoplasmic patterns. [7] The nuclear localization of ephrin A4 is explained by the ability of some tyrosine kinase receptors, with or without their ligand, to be transported to the nucleus. [10] The present study denied the previous speculation that the emergence of these unique patterns of ephrin A4 staining could be related to decalcification procedures, as the present specimens were incision biopsies not exposed to any types of decalcification. Our previous report suggested a different biological behavior between osteosarcoma cases that showed cytoplasmic pattern versus those showing both cytoplasmic and nuclear staining. [7] Therefore, in the present study, assessment of the prognostic value of ephrin A4 and its pattern of staining was mandatory, to clarify if there were true differences or not. In the present study, ephrin A4 was expressed in 82.9% of the primary osteosarcoma cases comparable to our previous result (84.4%), [7] but it is still lower than that reported by Varelias et al. 2002 (100%). [11] Statistically, there was no significant correlation between ephrin A4 expression and the clinicopathological parameters of the studied cases except for its tendency to be expressed in females more than in males (P = 0.08). Estrogens could have a role in the upregulation of certain types of ephrins such as EphB4 expression in the normal breast, which appeared to be dependant on estrogens. [12] The demonstration of estrogen receptor expression by malignant osteoblasts in osteosarcoma could point to the role of estrogens in this malignant tumor. [13] This may explain the observation of ephrin A4 expression by all females in our study. However, further studies are needed to investigate the correlation between estrogen receptors and ephrin A4 expressions in osteosarcoma. On the other hand, ephrin A4 expression in its cytoplasmic pattern of staining was associated with both progression and poor prognosis in primary osteosarcoma. This is manifested by the significant association of the cytoplasmic pattern with the aggressive types of osteosarcoma (MFH-like and fibroblastic types) (P = 0.02), advancement of TNM stage (P = 0.04), and with the presence of distant metastasis (P = 0.03). The cytoplasmic pattern of ephrin A4 was expressed in all cases of fibroblastic and MFH-like variants of osteosarcoma, in comparison with 52.9 and 30.8% of osteoblastic and chondroblastic osteosarcoma, respectively. The first two subtypes of osteosarcoma were aggressive lesions that were usually associated with local recurrence and metastasis. [14] The significant association of the cytoplasmic pattern of ephrin A4 with the advancement of the TNM stage could point to its role in osteosarcoma progression similar to the role of ephrin A1 in the advancement of urinary bladder carcinoma, [15] melanoma, [16] and ovarian carcinoma. [17] Furthermore, its association with the presence of distant metastasis indicates its role in promoting invasion and metastasis [18] and confirms our earlier observation of its exclusive expression in metastatic osteosarcoma lesions. [7] Conversely, the nucleocytoplasmic pattern was observed to be associated with a favorable prognosis, such as an early stage, absence of metastasis, and recurrence in osteosarcoma cases. This means that there was a different biological behavior between osteosarcoma cases with a pure cytoplasmic pattern and the other cases with the nucleocytoplasmic one. Whether the dominant localization of the ephrin A4 ligand in the cytoplasm means its full or maximum activity and the transportation of a part or the full ligand to the nucleus means deactivation or decrease in its biological activity remain to be elucidated in further studies. The majority agreed on the high prognostic value of the grade of histological response to chemotherapy manifested by the extent of tumor necrosis on patient outcome. [19] In our study, the only significant factor that predicts the preoperative chemotherapy response was the pattern of ephrin A4 staining. Ninety-five percent of our patients with cytoplasmic pattern showed inferior chemotherapy response (< 90% tumor necrosis). This could support our results that the cytoplasmic pattern of ephrin A4 staining was associated with tumor aggressiveness and poor outcome. Ephrins expression was associated with shorter overall survival together with shorter metastasis-free and event-free survivals in many malignant tumors suggesting that these molecules may have an impact on prognosis in different neoplasms such as cervical squamous cell carcinoma, [20] urinary bladder carcinoma, [15] ovarian carcinoma, [21] and breast carcinoma. [22] In our study, only a tendency of the cytoplasmic pattern of ephrin A4 (P = 0.09) to be associated with shorter event-free survival, is shown, supporting its role in enhancing invasion and metastasis. On the other hand, some authors reported that high levels of EphB4 and EphB2 expression were associated with a longer survival duration in colorectal carcinoma suggesting that they may act as tumor suppressor genes. [4] From this study, the cytoplasmic pattern of ephrin A4 could identify a subgroup of primary osteosarcoma patients with a high liability for progression, poor prognosis, and inferior response to chemotherapy. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10011t1.jpg] [cn10011f3.jpg] [cn10011f1.jpg] [cn10011t2.jpg] [cn10011f4.jpg] [cn10011f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}