 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
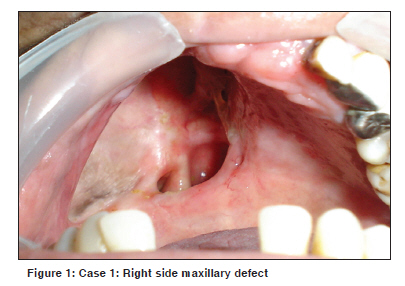
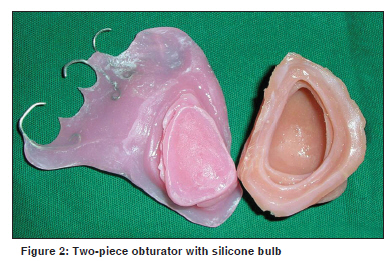
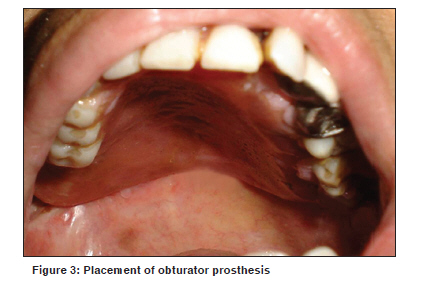
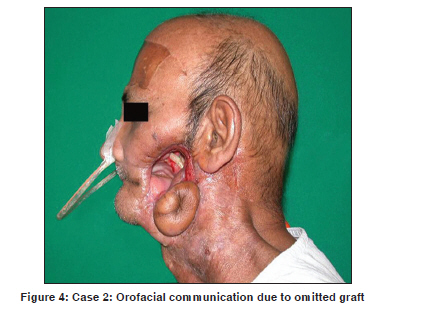
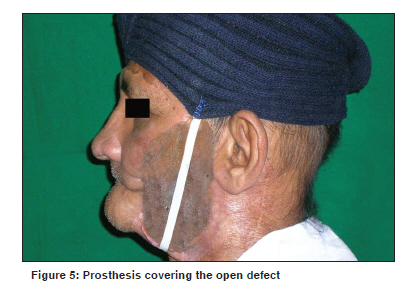
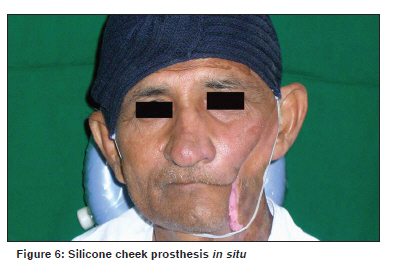
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 59-64 Brief Report Orofacial rehabilitation of patients with post-cancer treatment-An overview and report of three cases Guttal KS, Naikmasur VG, Rao CB1 , Nadiger RK2 , Guttal SS2 Departments of Oral Medicine and Radiology, 1 Oral and Maxillofacial Surgery, 2 Maxillofacial Prosthodontics, SDM College of Dental Sciences and Hospital, Sattur, Dharwad, India Code Number: cn10013 PMID: 20071792 DOI: 10.4103/0019-509X.58861 Abstract According to World Health Organisation statistics, individuals of the Indian subcontinent have the highest prevalence of orofacial cancer. Surgery, radiation, chemotherapy or combination therapies are commonly administered treatment modalities for treatment of oral cancer. Surgical resection can be mutilating, disfiguring and may deeply affect self-image of patients. Orofacial defects have unique limitations and challenges. A coordinated effort from the surgeon, oral physician and the maxillofacial prosthodontist to treat such patients is the need of the hour. This article presents an overview of the orofacial rehabilitation of postcancer treatments along with case reports.Keywords: Orofacial defects, oral cancer, rehabilitation, maxillofacial prosthesis Introduction Cancer of the orofacial region is one of the five leading sites of occurrences. Squamous cell carcinoma comprises 90%-95% among all orofacial cancers. [1] The primary treatment methods consist of local/regional therapy of surgery, radiation therapy or a combination of both modalities. [2] Patients with stage I and II disease have an excellent prognosis and have expected cure rates of 80% and 65%, respectively, [3] whereas patients with stage III or IV disease have poor prognosis. [4] Though surgery is the core treatment modality in the management of oral cancer, it fails to remain without development of complications. These include alteration in the clarity of speech, mastication and swallowing. This is related largely to loss of the mobile portion of the tongue, lack of clarity of articulation and bolus transport and mastication. The other sequelae of surgical treatment are related to external appearance and wound contracture. Transoral laser microsurgery is a new trend for complete resection of accessible lesions, [5] but it is time consuming, technically demanding and requires a larger number of new instruments. Reported cure rates are comparable to historical cure rates. [6],[7],[8] Initial surgical resection followed by radiotherapy or chemotherapy is commonly selected for resectable oral cavity tumors. [9],[10],[11],[12] Currently, the use of concurrent chemoradiotherapy has been suggested for the treatment of orofacial cancers. Chemotherapy is believed to synergistically act with radiotherapy by inhibiting repair of DNA damage caused by radiotherapy, arresting cells in radiosensitive phases and possibly preventing regrowth between radiotherapy treatments. [13] Treatment of side effects during this period is supportive and symptomatic. It is always advisable to have a thorough oral examination done by an oral physician before the start of the radiation therapy. On the basis of presenting situation, the decayed or periodontally compromised teeth, can either be treated conservatively or extracted before the radiation therapy. [14],[15],[16] Postoperative management of patients involves a coordinated approach by a multidisciplinary team of medical and radiation oncologist, oral and maxillofacial surgeon, oral physician, prosthodontist, dietician and physical therapist. [17] The role of a prosthodontist cannot be overemphasized in the replacement of lost orofacial structures even prior to surgery. This facilitates planning of surgery and accurate replacement of missing parts to simulate the normal. The prosthetic restoration of missing oral and facial structures is indicated when surgical procedures cannot be expected to produce satisfactory functional or cosmetic results. Presented here are few case reports of the patients treated with prosthetic restoration of the missing oral and facial parts following treatment of cancer. Prosthetic rehabilitation restored the function and psychological set back, thereby improving the quality of life of the patients. Cases Case 1 A 45-year-old female patient was referred to the Department of Maxillofacial Prosthodontics, with the complaint of inability to swallow due to the oronasal communication [Figure - 1]. The patient had undergone maxillectomy of the right side due to squamous cell carcinoma and had limited mouth opening. Owing to the large defect, a two-piece obturator prosthesis was planned, which had the detachable silicone bulb and the acrylic resin prosthesis replacing the missing teeth. The prosthesis gained retention primarily from the clasps engaging the undercut on the abutment teeth and secondarily the silicone bulb engaged the undercut from the defect. With the placement of the obturator prosthesis, physical separation between oral and nasal cavities was achieved. The patient had improved function in terms of mastication, deglutition and speech. The prosthesis also improved the psychological status as well as quality of life of the patient. Insertion and removal of large prostheses used for rehabilitation of midfacial defects requires good neuromotor coordination and an adequate mouth opening. Both these factors were unfavorable for the patient and could have compromised the prognosis of the treatment. Hence, a two-piece obturator was designed [Figure - 2]. The two-piece prosthesis helped in easy removal and placement of the prosthesis [Figure - 3]. Case 2 A 55-year-old male patient was diagnosed with squamous cell carcinoma of the left buccal mucosa and involving the alveolus of the same side. Surgical treatment resulted in an orofacial communication [Figure - 4]. Surgical reconstruction was done using the forehead skin graft. Unfortunately the graft was omitted and the tissue contraction and scarring formed a lump near the lower border of the mandible. Later, the patient was referred to the prosthetic treatment for the restoration of the defect. The patient's chief complaint was the escape of food and fluids through the orofacial communication. The dehiscence defect was found on the left cheek and the patient expressed his desire to have a prosthesis that would improve function and esthetics. The defect was packed with lubricated gauze to prevent intrusion of the impression material into the oral cavity. The defect impression was made using irreversible hydrocolloid. The prosthesis was waxed to form. It was verified on the patient's face during the try-in appointment, and minor corrections to the wax-up were made. The waxed prosthesis was invested and the mold prepared. Intrinsically colored silicone was packed into the mold. The silicone cheek prosthesis was retrieved and finished. The prosthesis was placed on the patient [Figure - 5]. It was retained using elastic straps that were attached to the head cap [Figure - 6]. The prosthesis was found to be seated well with an effective seal during function. Follow-up was done once in a month for six months and the patient had no complaints. Case 3 A 58-year-old female patient was referred to the aforementioned department with the patient complaint of missing left orbital contents [Figure - 7] following the surgery due to adenoid cystic carcinoma. Examination revealed that the defect was placed with a skin graft taken from the forehead. The patient was seeking cosmetic replacement of the lost eye. A custom-made ocular and orbital prosthesis was planned and the treatment procedure was explained to the patient. Irreversible hydrocolloid impression was made and the stone cast was poured. Orbital wax pattern was made on the resultant cast. A trial of waxed prosthesis was taken. The wax prosthesis was invested and the mold prepared. It was packed with intrinsically colored silicone. The silicone orbital prosthesis was placed in situ. The prosthesis was retained with the help of the spectacle glass frame [Figure - 8]. Follow-up evaluation was done for once in a week for 2 months and the patient was satisfied with the esthetic outcome of the prosthesis. Discussion Cancer of the head and neck region can profoundly affect the quality of life (QOL) of patients, as they are constantly reminded of their affliction. The prosthodontist and the oral physician play an important role in the prevention, stabilization and treatment of oral and dental problems that can compromise the health and quality of life of patients with cancer during and after the cancer treatment. Patients with head and neck cancer often suffer from cancer cachexia. The physiologic mechanism for this state of anorexia, weight loss and tissue wasting includes metabolic, obstructive and treatment-related factors. The side effects of all forms of antineoplastic therapies contribute to development of malnutrition. The unaddressed odontogenic infections may further complicate the situation, rendering the patient to extended psychological trauma and loss of compliance for follow-up. Moizan et al.[18] used a questionnaire among 164 practitioners to evaluate the dental treatments and related ethical considerations. They concluded that the absence of a dental consultation reduced the preventive care and prosthetic rehabilitation of patients, thereby reducing the quality of life for these patients. The patients incurring extensive defects of the oral and facial structures need prosthetic rehabilitation fulfilling the objectives such as function, esthetics and prevention of infection. Prosthetic rehabilitation of postoperative cancer patients is classified as (1) intraoral and (2) extraoral rehabilitation. Intraoral Prosthetic Rehabilitation This includes the obturators for the maxillary defects and the guide flange prosthesis for the mandibular defects. Obturators are of three types: (1) Surgical, (2) Interim and (3) Definitive. Surgical obturators are prepared before surgery and inserted in the operating room at the time of surgery. The prosthesis can be ligated to the remaining teeth with wire or retained with a bone screw in the edentulous patient. This obviates the necessity for using a nasogastric tube, and allows the patient to speak and swallow immediately after surgery. [19],[20],[21] Interim obturators are constructed one to two weeks after surgery. As the wounds of patients heals, it is necessary to revise the obturator periodically to maintain a velopharyngeal seal. This is achieved with the use of a resilient liner. [20] The definitive prosthesis is made when the tissues are well healed and dimensionally stable. Reconstruction of the maxilla with a flap or an obturator seems to be relative. Various surgical techniques have been advocated for reconstruction, including the temporalis flap, the osteocutaneous scapula flap, and vascularized free flaps. [22],[23],[24],[25],[26],[27],[28] Ali et al.[29] conducted a questionnaire study among the British oral and maxillofacial surgeons to know whether postmaxillectomy defects may be restored either by surgical reconstruction or by prosthesis. They concluded that 38% of the surgeons perform surgical reconstruction and 62% of them refer to a prosthodontist for prosthesis. Minor maxillary defects can be surgically repaired using regional flaps or free-tissue transfers. [21] Surgical reconstruction depends on the size and location of the defect. Reconstruction is usually limited by the availability of tissue, damage to the local vascular bed and the need for periodic visual inspection of the oncologic defect. It is preferred for small defects whether it is an extraoral facial defect or an intraoral maxillary defect. In large extraoral and intraoral defects, surgical reconstruction often provides limited functional results. In case 1, the silicone bulb was fabricated due to the limited mouth opening. Literature reports reveal similar design of the obturator prosthesis, [30] with the hollow bulb being fabricated with acrylic resin and the surface of the resin frame layered with silicone. The denture portion and the bulb were aligned using magnets. In this case, the entire bulb was fabricated using silicone. This made the prosthesis light in weight compared with the previously reported design, with the absence of acrylic resin frame. The lightness of the obturator improves the fundamental problem of retention and increases physiological function by applying less stress on teeth and supporting tissues, thereby preventing excessive atrophy and physiological changes in muscle balance. [31],[32],[33] According to Desjardins, [34] there are five intrinsic areas within and around the defect that can provide retention for the obturator. These areas include the residual soft palate, the residual hard palate, the anterior nasal aperture, the lateral scar band and the height of the lateral wall. The silicone obturator engaged the defect undercut by adapting very well to the walls of the defect. This increased the retention and stability of the prosthesis. The patient was satisfied with treatment since there was no fluid leakage into the nasal cavity. During the follow-up appointment the patient expressed the remarkable improvement in the speech and prosthesis comfort because of the soft silicone bulb. Extraoral Prosthetic Rehabilitation Extraoral prosthesis is the facial prosthesis that includes the replacement of any missing part of the face. The orbit, nose and ear are the facial prostheses that are retained usually by extraoral implants, adhesives or by the conventional methods. When there is communication between intraoral and extraoral defects resulting from surgery, the facial portion of the prosthesis can be retained via its attachment with intraoral component. The area in which the prosthesis is to be placed should have stable tissue base for better support, which can be achieved by the placement of split-thickness skin graft. The graft also provides retention by tolerating the tissue adhesives used to retain facial prosthesis and will improve hygiene. [35] In case 2, the patient had a large defect on the left side of the cheek, creating an orofacial communication. The defect was closed by cheek prosthesis. The prosthesis was prepared using silicone material, which reproduces the life-like appearance. Functional relining was done to achieve the facial seal. The effectiveness of the seal was evaluated by asking the patient to sip water and no leakage of water was observed during the act. The prosthesis was retained with the help of elastic band attached to the head cap. Additionally, the head cap also masked the scar of the forehead, which was the source of skin graft. In case 3, the entire orbital contents were surgically removed due to cancer. The bony structures of the orbit were left intact and all the margins were rounded off at the conclusion of the surgery. Thus, there was better adaptation of the silicone orbital prosthesis margins to the defect. Conventionally, retained orbital prostheses are practical, trouble-free, cost efficient and successful. [36] The most commonly used conventional method to retain orbital prosthesis is the eyeglass frame and anatomic retentive undercuts. The patients' defect had no undercuts; hence, an eyeglass frame was the only alternative to retain the silicone orbital prosthesis economically. The patient was wearing the prosthesis routinely and was satisfied with the cosmetic results. Osseointegrated craniofacial implants enhance the retention of the facial prostheses and improve patients' self confidence and acceptance with treatment. [37],[38] Financial constraints form a major setback for patients to opt for the implant-retained prosthesis. Success rates of osseointegrated implants used to restore craniofacial defects is excellent. [39],[40] However, the survival of implants placed in the irradiated bone is questionable. [41] Summary Surgery, radiation and chemotherapy are used in the management of orofacial cancers. Surgical resection often creates large defects accompanied by dysfunction and disfigurement. Speech, swallowing, inability to control saliva secretions and cosmetics can be adversely affected. The management of a patient with cancer does not conclude with elimination of the disease but continues with rehabilitation of function, restoration of esthetics and prevention of infection and maintenance of proper oral hygiene. A planned coordination among the surgeon, oral physician and the prosthodontist is essential preceding the surgery. This facilitates harmonization of the surgical techniques with the prosthetic procedures. The oral physicians' consultation will guide the patients to manage the complications of chemoradiotherapy. Prosthetic rehabilitation of extraoral and intraoral defects significantly reduces the psychologic morbidity. References
Copyright 2010 - Indian Journal of Cancer |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}