 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
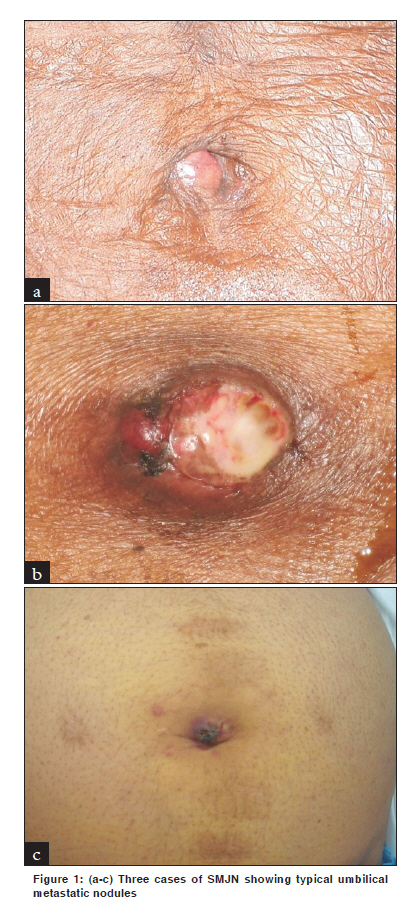
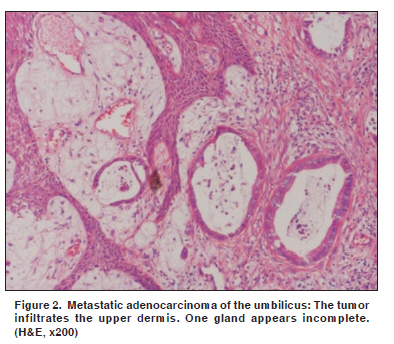
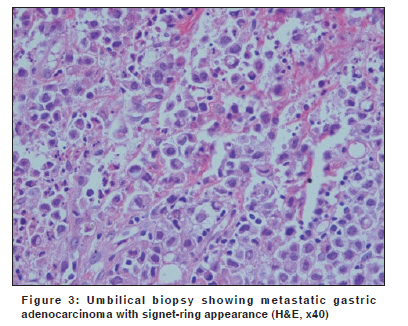
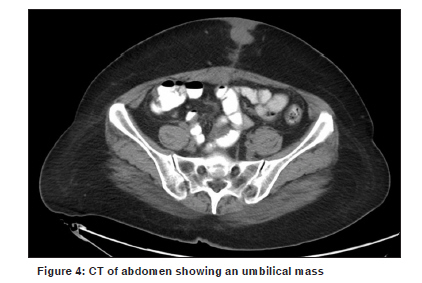
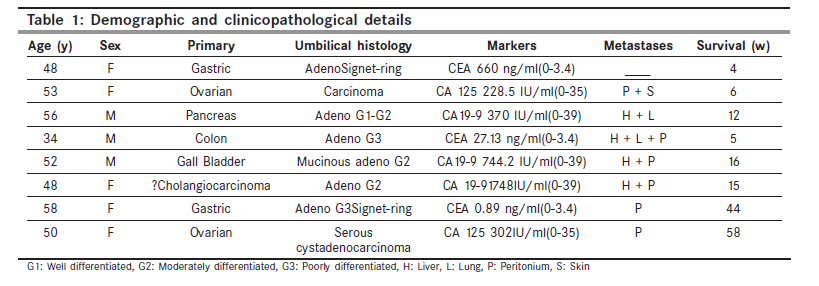
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 65-69 Brief Report Sister Mary Joseph's nodule of the umbilicus: Is it always of gastric origin? A review of eight cases at different sites of origin Al-Mashat F, Sibiany AM Department of Surgery, King Abdulaziz University Hospital, College of Medicine, King Abdulaziz University, Jeddah, Saudia Arabia Code Number: cn10014 PMID: 20071793 DOI: 10.4103/0019-509X.58862 Abstract Objective : The aim of this analysis was to evaluate our management and outcome of eight cases of Sister Mary Joseph's Nodule of the umbilicus (SMJN). Methods : Between 2002 and 2009, we collected eight cases of SMJN and their clinical data were studied in a retrospective manner. Results : The mean age of the patients was 50.6 years (range, 34-58). There were three males and five females. Five cases were discovered preoperatively during an abdominal examination and in the remaining three patients, the umbilical nodule was noticed during surgery. Most patients presented with abdominal pain. Various signs were discovered during clinical examination. Exhaustive investigations done included ultrasound, computed tomography, magnetic resonance imaging, endoscopic retrograde cholangiopancreatography, magnetic resonance cholangiopancreatography, gastrointestinal endoscopy, mammogram, bone scan, and a panel of tumor markers. The primary tumors were gastric adenocarcinoma (two patients), ovarian adenocarcinoma (two patients), pancreatic carcinoma (one patient), colonic adenocarcinoma (one patient), gallbladder adenocarcinoma (one patient), and cholangiocarcinoma (one patient). As the disease was advanced and metastatic in all patients, only palliative therapy was offered. All patients died within a short period after clinical presentation, ranging from four to 58 weeks (mean, 20 weeks). Conclusion : SMJN is a rare manifestation of a variety of advanced malignancies, usually of gastrointestinal origin. A majority of the patients present at a late stage and many harbor distant metastases. The patient's survival is very short (mean, 20 weeks) leading to a poor outcome. We believe that if the primary cancer is discovered at an early stage, the prognosis may improve.Keywords: Sister Mary Joseph's Nodule, umbilical metastasis, umbilical deposit following laparoscopic cholecystectomy Introduction Sister Mary Joseph's Nodule of the umbilicus (SMJN) is a metastatic tumor deposit in the umbilicus, the anatomical region where the peritoneum is closest to the skin. Classically, it is associated with intra-abdominal epithelial tumors, and often represents advanced malignancy with dismal prognosis. [1] The most common primary source is the gastrointestinal tract (35 - 65%), followed by the genitourinary tract (12 - 35%). [1] In 15 - 30% of the patients the source of the primary tumor remains unknown. [2],[3],[4] This sign may be the first clinical manifestation of cancer or indicates tumor recurrence. We report eight cases of SMJN originating from the stomach, ovary, pancreas, sigmoid colon, gallbladder, biliary tree. The patients received only palliative surgical intervention and adjuvant chemotherapy, as they had locally advanced and / or metastatic tumors. The eight patients survived for a very short period (4 - 58 weeks) after clinical presentation. Methods The files of eight patients with SMJN were studied. These patients were seen at two teaching hospitals from May 2003 to May 2009. In all the patients the diagnosis of umbilical metastasis was confirmed histologically. Also, the primary carcinoma was confirmed histologically in seven patients. The data collected included age, gender, symptoms, signs, size of umbilical nodules, timing of discovery of nodules, investigations carried out to look for the primary cancer, sites of origin of primary cancer, therapeutic options, and duration of survival. Six patients had been followed up in the Outpatient Departments and their death was documented. Two patients were lost to follow-up and their date of death was obtained from relatives. Results The mean age of eight patients with SMJN was 50.6 years (range, 34 - 58). There were five female and three male patients. Common presentations included abdominal pain, weight loss, constipation, and vomiting. Clinical examination revealed epigastric mass, pelvi-abdominal mass, and ascites in two patients each and hepatomegaly and left iliac fossa mass in one each. The umbilical nodules were tender and ulcerated in three patients, hard in all, and their sizes varied between 2 and 4 cm (mean, 2.9 cm) [Figure - 1]a-c. The nodule was discovered at the initial clinical examination in five patients and in the other three patients it was noticed during surgery. One patient developed metastatic umbilical adenocarcinoma three months after laparoscopic cholecystectomy. The nodule recurred in two patients after complete excision. The recurrent nodule was excised in one patient because it was painful and measuring 15 cm. The diagnosis of SMJN was confirmed in all patients by umbilical biopsy, and a histopathological review showed various malignancies metastasizing to the umbilicus [Figure - 2] and [Figure - 3]. Searching for the primary cancer was aided by gastrointestinal endoscopies, imaging modalities, and a panel of tumor markers. CT detected SMJN in all patients [Figure - 4] and in one patient the nodule was seen during US examination of the abdomen. A panel of tumor markers in the serum complemented the search for the primary cancer and included a carcinoembryonic antigen (CEA), CA 19-9, CA 15-3, CA 125, and alpha fetoprotein (AFP). Diagnosis of the primary cancer was confirmed in six patients by biopsy and in one patient after bilateral salpingo-oophorectomy and hysterectomy. The diagnosis of cholangiocarcinoma in the eighth patient was strongly suspected by CT, ERCP, and MRCP in spite of negative brush cytology. The primary sites were gastric (two patients), ovarian (two patients), colon (one patient), pancreas (one patient), gall bladder (one patient), and cholangiocarcinoma (one patient). [Table - 1] shows the demographic and clinicopathological details. Surgical interventions done were of a palliative nature, without curative intent, as all patients had either locally advanced or metastatic disease. Chemotherapy was given to two patients with colon and ovarian carcinoma. The patients survived for only a few weeks after clinical presentation with SMJN. They survived for a mean period of 20 weeks (mean, 4 - 58). The longest survival was noticed in a patient with serous cystadenocarcinoma of the ovary (58 weeks). Discussion Sister Mary Joseph (1856 - 1939), superintendent of St. Mary's Hospital, now known as Mayo Clinic, was the first surgical assistant under the guidance of Dr. William Mayo, serving in this capacity from 1890 to 1915. [5] During this period, while preparing patients with gastric cancer for surgical resection, Sister Joseph noted the presence of a firm mass at the umbilicus in individuals who invariably had a poor outcome and succumbed relatively early postoperatively [6] Dr. Mayo first reported the condition as "pants-button umbilicus" (without credit to Sister Mary Joseph) in a lecture to the Cincinnati Academy of Medicine in 1928. [7] The first case reporting the presence of SMJN was in 1864 by Storer. [8] The term SMJN did not exist, however, until 1949, when Hamilton Bailey coined the term in the eleventh edition of his textbook, 'Physical Signs in Clinical Surgery.' [5] Cutaneous metastases are rare and range between 5 - 9%. It is estimated that 1- 3% of Abdominopelvic tumors metastasize to the umbilicus. [9],[10],[11] SMJN is a rare clinical entity and represents only 10% of all cutaneous metastases. [9],[12] It often presents as the first sign of intra-abdominal malignancy, usually represents an advanced disease, and carries a very poor prognosis. [13] Because the nodule is so easy to biopsy and because most associated cancers are inoperable at the time of diagnosis, the ability to identify this lesion may save a patient an unnecessary diagnostic surgery. [9] SMJN constitutes 83% of all malignant umbilical tumors, being much more common than primary malignant umbilical tumors. [9],[10],[14] The most common histological type is adenocarcinoma (75%), more rarely squamous cell carcinoma, undifferentiated tumors, carcinoid, sarcoma, mesothelioma, melanoma, and lymphoma. [8],[15],[16],[17] The gastrointestinal tract is the most common location of the primary neoplasm (35 - 65%), followed by a gynecological origin (12 - 35%). [1] The common sites in decreasing order of frequency are: stomach (25%), colorectal (10%), and pancreas (7%). [5] In females, ovarian cancer is the most common primary site, of which serous papillary cystadenocarcinoma is the most frequent (34%). [8] Primary tumors in many other sites have been reported to lead to SMJN, including gallbladder, liver, breast, lung, prostate, penis, peritoneum, lymphoma, bladder, kidney, endometrium, cervix, vagina, vulva, and fallopian tube. [5],[8] In 15 - 30% of the cases, the source of the primary site of the tumor is unknown [2],[3],[4] In approaching a patient with SMJN, potential benign causes must be considered, including endometriosis, melanocytic nevi, fibroepithelial papillomas, dermatofibroma, fibroma, epithelial inclusion cyst, urachal duct cyst, seborrheic keratosis, pilonidal sinus, keloid, foreign body, granuloma, myxoma, omphalitis, polyp, abscess, and hernia. [5],[8],[9],[18] Additional differential diagnosis include primary malignant umbilical tumors, which are exceedingly rare, accounting for 17% of the cases and include melanomas, basal cell carcinomas, squamous cell carcinomas, myosarcomas, and adenocarcinomas. [9] The spread of metastatic cancer to the umbilical region has been postulated to occur in several ways. These include direct extension from a contiguous tumor (the most important), hematogenous (arterial and venous), lymphatic and direct extension along the vestigial remnants of embryonal ligaments including the round ligament, the urachus, the vitellointestinal duct remnant, and the obliterated vitelline artery. [18],[19],[20] In addition, direct implantation following laparoscopy is another mode of spread of tumors to the umbilicus. [21] The clinical appearance is often that of a painful lump with irregular margins and hard consistency. The surface may be ulcerated and necrotic with either blood, serous, purulent, or mucous discharge from it. The size of the nodule usually ranges from 0.5 - 2 cm, although some nodules may reach up to 10 cm in size. [1],[10] Various imaging modalities can aid in establishing the diagnosis such as Ultrasonography (US), Computed tomography (CT), Magnetic resonance imaging (MRI), and Positron emission tomography (PET). Once SMJN is discovered, a biopsy, either excisional or fine needle aspiration (FNA), is mandatory to establish diagnosis and to find the possible primary site. The histopathologic evaluation may show characteristics of the underlying tumor, or they may have a more anaplastic appearance. In the situation of an anaplastic tumor, immunohistochemical marker studies and ultrastructural examination may help delineate the tissue of origin. [22] The presence of SMJN usually signifies an advanced, metastasizing cancer, and therefore, a poor prognosis. The finding of a metastatic nodule at the umbilical site almost certainly establishes the inoperability of the patient. [23] This conclusion of Clements was disputed by others who believe that the existence of SMJN is insufficient proof of widespread metastatic disease that would prevent an operation. Uncommonly, SMJN may represent a solitary metastasis or possibly a primary tumor that has not yet metastatized. [24],[25] SMJN usually represents widespread metastasis and treatment is commonly palliative. Several authors have advocated wide excision with extensive search for the primary lesion, [25],[26] radiotherapy, [27] and surgery with adjuvant therapy. [20] Majmudar has shown that patients treated aggressively with both surgery and adjuvant therapy live for an average of 17.6 months, which is more than with surgery alone (7.4 months), adjuvant therapy alone (10.3 months), or no treatment (2.3 months). Aggressive surgical approach combined with chemotherapy may improve survival. [1] Excellent response to systemic therapy was achieved in non-Hodgkin's lymphoma. [17] If SMJN causes ulceration or disfigurement, local excision is warranted, to improve the quality of life. All our eight patients died after an interval of 4 - 16 weeks (mean, 9), without our offering them any curative therapeutic modality. This very short survival is in keeping with the advanced and metastatic nature of the primary cancer. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10014f2.jpg] [cn10014f4.jpg] [cn10014f1.jpg] [cn10014t1.jpg] [cn10014f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}