 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
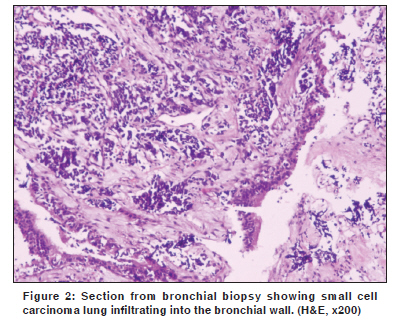
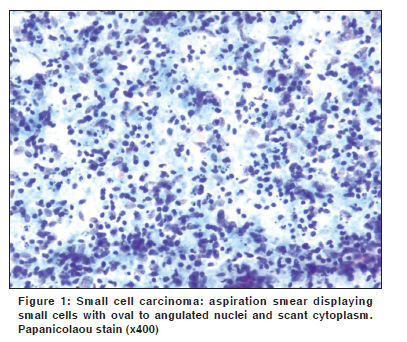
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 72-73 Letter To Editor Metastatic small cell carcinoma lung presenting as a breast mass: Cytologic findings Sharma S, Kotru M University College of Medical Sciences, Delhi, India Code Number: cn10017 PMID: 20071796 DOI: 10.4103/0019-509X.58865 Sir, Most malignancies seen in the breast are primary carcinomas. Metastasis to the breast from extramammary primary malignancies is rare and usually part of disseminated malignancy. We report a case of multiple breast metastases from a known case of carcinoma lung presenting with superior venacaval syndrome. A 45-year-old lady presented with history of dyspnea associated with cough for 6 months. On examination, the patient had neck and facial swelling with dilated neck veins. There was a hard left cervical mass measuring 3 cm x 2 cm. Examination of the breast revealed two lumps on the left side. The larger lump was 4 cm x 3 cm, hard and irregular in the outer quadrant of the breast. Chest radiograph showed a left hilar mass, which was confirmed on computed tomography scan. Bronchial biopsy revealed a small cell carcinoma infiltrating into the bronchial wall [Figure - 2]. There was no history of smoking. Fine needle aspiration was performed from both breast lumps and left cervical mass. All the smears were highly cellular and revealed pleomorphic cells arranged in loose clusters with a high N:C ratio and round to oval hyperchromatic nuclei showing moulding and inconspicuous nucleoli [Figure - 1]. In view of cytological findings and clinical features, an impression of small cell carcinoma lung metastasizing to breast was given. The patient was advised radiotherapy and chemotherapy, which she refused and was lost to follow-up. Metastatic tumors to the breast (excluding hematopoietic malignancies) are relatively rare (0.5-2% of all malignant breast tumors). The malignant neoplasm that most commonly metastasizes to a breast is primary disease of the contralateral breast. [1],[2] One of the most common occult primary tumor sites is the lung. [2] Other clinically occult neoplasms that may present with breast metastases include malignant melanoma, carcinoma of kidney and stomach. [3] The most common finding is a painless lump in the upper outer quadrant and 80% of patients have a known diagnosis of non-mammary malignancy at the time of presentation of breast lump.[4] In our case too, because the patient had a 6-month history of lung symptoms followed by biopsy-proven small cell carcinoma of the lung, the possibility of metastases was considered first. Radiologically, metastases tend to be discrete round shadows without speculation and are not distinguishable from papillary, medullary or colloid primary breast carcinomas. [3] The distinction of primary breast malignancy from metastases on cytohistology is based on features not usually seen in primary tumors of breast, such as intra-cytoplasmic pigment (melanin), small undifferentiated cells (small cell carcinoma lung) and hematopoietic cells. [5] Difficulty arises in tumors with similar morphologic pattern as primary carcinoma of the breast. In our case, the striking small cell morphology led us to propose the diagnosis of metastatic small cell carcinoma of lung. Immunohistochemistry can be useful to distinguish primary breast tumor from metastases, depending on the suspected primary tumor. However, because small cell carcinoma of both breast and lung show similar immunochemical pattern, it was not useful in our case. [5] Metastatic disease to the breast, although not considered in the initial workup of a patient with breast lump, should rouse suspicion of metastasis in a case of known primary malignancy elsewhere. Also, the possibility of metastasis should be suspected in lesions with unusual cytologic patterns (like melanoma and small cell carcinoma). References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10017f2.jpg] [cn10017f1.jpg] |
| |||||||||

{kind=link}
{kind=link}