 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
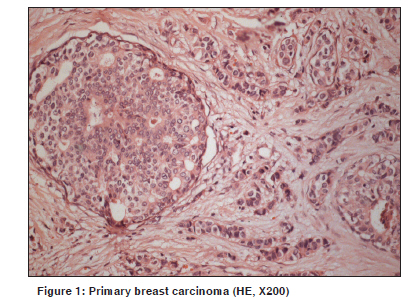
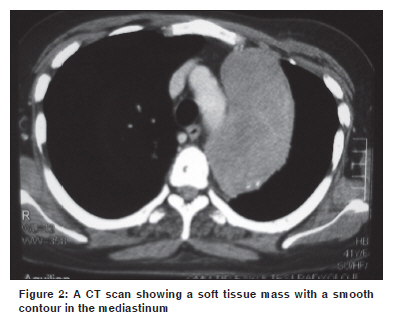
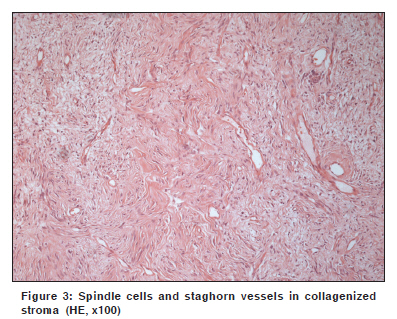
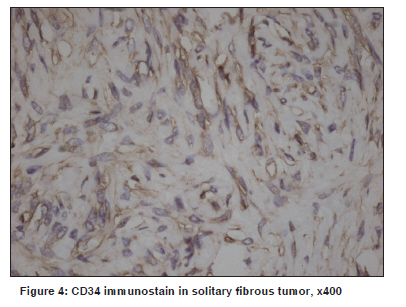
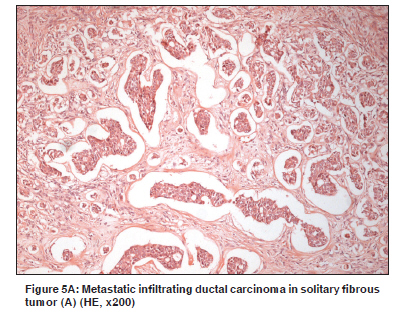
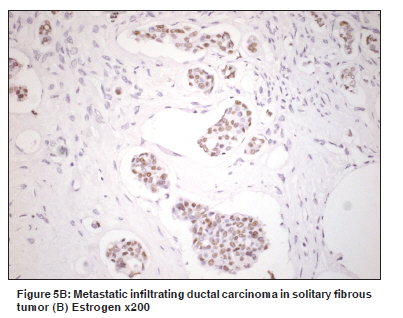
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 76-78 Letter To Editor Metastatic breast carcinoma to solitary fibrous tumor in the lung Gönüllü G, Süllü Y, Başoğlu A, Elmalı M, Karaoğlanoğlu M, Yücel İ Ondokuz Mayis University Medical School, Department of Medical Oncology Kurupelit, Samsun, Turkey Code Number: cn10020 PMID: 20071799 DOI: 10.4103/0019-509X.58868 Sir, A 41-year-old woman was admitted to the hospital with a mass in the left breast. Excisional biopsy revealed 'infiltrative ductal carcinoma' [Figure - 1]. A chest x-ray showed a mass in the left lung apex. Bronchoscopy was performed. There was no endobronchial lesion. Bronchial washing was negative for malignancy. Thorax CT demonstrated a 10 x 7 x 10 cm soft tissue mass with a smooth contour, which started from the left upper mediastinum and extended to the middle and posterior mediastinum. The mass was near the aortic arch, descending aorta, and left pulmonary artery [Figure - 2]. The mass was totally removed. Histopathological examination disclosed a neoplasm composed of spindle cells that were arranged in a fascicular pattern or haphazardly in dense collagenized stroma. The stroma was rich with staghorn-shaped branching vessels. Nuclear atypia and mitoses were not observed. Within the tumor, there were also atypical epithelial cell islands, some of which formed ducts. The spindle cells were diffusely positive for CD-34 and vimentin, focally positive for smooth muscle actin (SMA), and negative for cytokeratin S-100 and mesothelial cell markers. The epithelial area was positive for cytokeratin, estrogen, and progesterone receptors and negative for vimentin, mesothelial cell markers, and CD34 [Figure - 3],[Figure - 4],[Figure - 5A, B]. The mediastinal pleura near the mass was not involved by tumor, but there was breast carcinoma infiltration of the posterior thoracic wall and parietal pleura. Osteoblastic activity was observed at the costovertebral junction and the left acetabulum. The patient was treated with radiation therapy followed by six cycles of chemotherapy (docetaxel + doxorubicine) and endocrine therapy for 24 months. Neoplasms frequently seen as donors in tumor-to-tumor metastases include carcinomas of the lung, breast, and prostate. Tumors that act as recipients are usually renal cell carcinomas, meningiomas, thyroid neoplasms, and pituitary adenomas. The tumor's metastatic ability is related to factors such as the production of enzymes like collagenase, loss of expression of adhesion molecules, expression of soluble adhesion molecules by tumor cells, and production of peptides that stimulate angiogenesis. Breast cancer, like melanomas and lung cancer, can metastasize to other tumors. The metastasis to an organ or another tumor is related to anatomic location, vascularity, and the local immune response to the tumor.[1],[2] Solitary fibrous tumors, like renal cell carcinomas are tumors suitable for metastasis because of their rich vascularity. According to Campbell, [3] the criteria are as follows: (a) more than one primary tumor must exist; (b) The recipient tumor is a true benign or malignant neoplasm; (c) The metastatic neoplasm is a true metastasis, with established growth in the host tumor, and not the result of contiguous growth or embolization of tumor cells, and (d) tumors that have metastasized to the lymphatic system where lymphoreticular malignant tumors already exist, are excluded. The spindle cells in a solitary fibrous and desmoid tumor are strongly and diffusely positive with CD34, whereas, the spindle cells in synovial sarcoma and mesothelioma are negative for this marker. The spindle cells are negative for a number of epithelial markers, including epithelial membrane antigen (EMA) and cytokeratin, which are typically positive in synovial sarcomas. [4] In conclusion, although tumor-to-tumor metastasis occurs infrequently, this possibility should always be considered References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10020f5a.jpg] [cn10020f2.jpg] [cn10020f5b.jpg] [cn10020f3.jpg] [cn10020f4.jpg] [cn10020f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}