 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
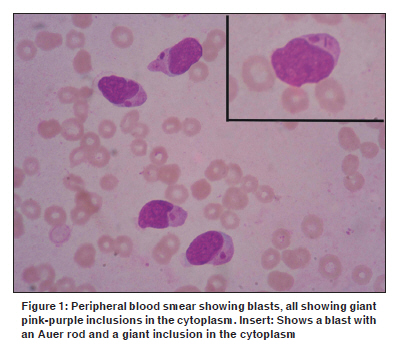
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 81-82 Letter To Editor Pseudo Chediak Higashi inclusions in a patient with acute myeloblastic leukemia Kakkar N, Das S, Joseph JM1 Departments of Pathology and 1Clinical Hematology, Christian Medical College & Hospital, Ludhiana, Punjab, India Code Number: cn10023 PMID: 20071802 DOI: 10.4103/0019-509X.58871 Sir, Giant cytoplasmic inclusions in myeloblasts or myeloid precursors, resembling those seen in the Chediak Higashi Syndrome (CHS), are called pseudo Chediak Higashi inclusions. It is a rare occurrence, with only sporadic reports in the literature. [1],[2] We report a patient with acute myeloid leukemia with these inclusions. A 21-year-old woman presented with fever and bleeding from the gums, since four days. On examination, she had pallor, left cervical lymphadenopathy, and mild hepatosplenomegaly. Investigations showed hemoglobin of 2.3 gm/dl (normal - 12.0 - 15.0 gm/dl), white cell count of 110 x 10 9 /l (normal - 4.0 - 11.0 x 10 9 /l), and platelet count of 15 x 10 9 /l (normal: 150 - 400 x 10 9 /l). Differential leukocyte count showed 95% blasts of size 14 - 20µ, immature nuclear chromatin, and 1 - 3 conspicuous nucleoli. The cytoplasm in most of the blasts contained purple, mostly single giant inclusions (1 - 3µ) [Figure - 1]. Rare blasts showed both Auer rods as well as inclusions [Figure - 1, Insert]. The inclusions were strongly positive for Myeloperoxidase and Sudan black. The Periodic Acid Schiff stain was negative. A bone marrow aspirate showed 92% blasts. The aspirate smears and trephine biopsy did not show the presence of inclusions. Bone marrow cytogenetics was normal. Immunophenotyping was not done due to the presence of Auer rods in the peripheral smear, which confirmed the myeloid nature of the blasts. The patient was given 3 + 7 induction therapy with Daunorubicin (45 mg/m 2 ) and Cytosine (200 mg/m 2 ). Day 14 bone marrow showed no residual disease. However, due to severe fungal pneumonia and septicemia she succumbed due to respiratory failure, by day 24. Pseudo-Chediak Higashi inclusions are proposed to be formed by a fusion of smaller granules and considered to be abnormal peroxidase positive variants (lacking sulfated glycoaminoglycans) of the primary granules, unlike the lysosomal origin of granules in CHS. Previous reports of these inclusions have shown consistent myeloperoxidase positivity and variable positivity for acid phosphatase and High Iron Diamine. On electron microscopy, the granules showed electron-lucent material with a dense matrix and occasionally "fingerprint" structures at the periphery. The giant granules were different from the large granules of CHS, as they contained numerous microcrystalline structures like those of the Auer bodies. [1] A study has also shown frequent CD2 expression in the myeloblasts with pseudo Chediak Higashi granules. [3] The association of a rare translocation t (10; 11) (p13; q14) has also been shown in a patient with AML-M5a, with myeloblasts containing pseudo Chediak-Higashi granules. [4] Previous reports on these inclusions describe them to be pink, azurophilic, or having a vacuolated appearance with myeloperoxidase positivity. [1],[3],[4],[5] The inclusions in our study had a purple appearance and were myeloperoxidase positive. Chediak Higashi syndrome usually presents in infancy or early childhood, classically with oculocutaneous albinism, silvery hair, and bleeding diathesis. Our patient was older, with no history of consanguinity or recurrent infections. Although our patient had inclusions resembling those seen in CHS, they were more prominent in the peripheral blood than in the bone marrow. Both conditions are distinct entities and are not related. The clinical significance of these inclusions is unclear. However, it is interesting to note that a feature that is otherwise seen in a congenital disorder has been acquired in AML. Further molecular studies are required to establish the therapeutic and prognostic relevance of this finding. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10023f1.jpg] |
| |||||||||

{kind=link}