 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
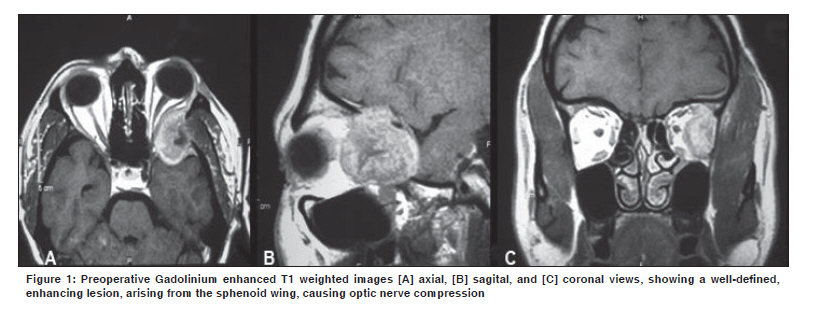
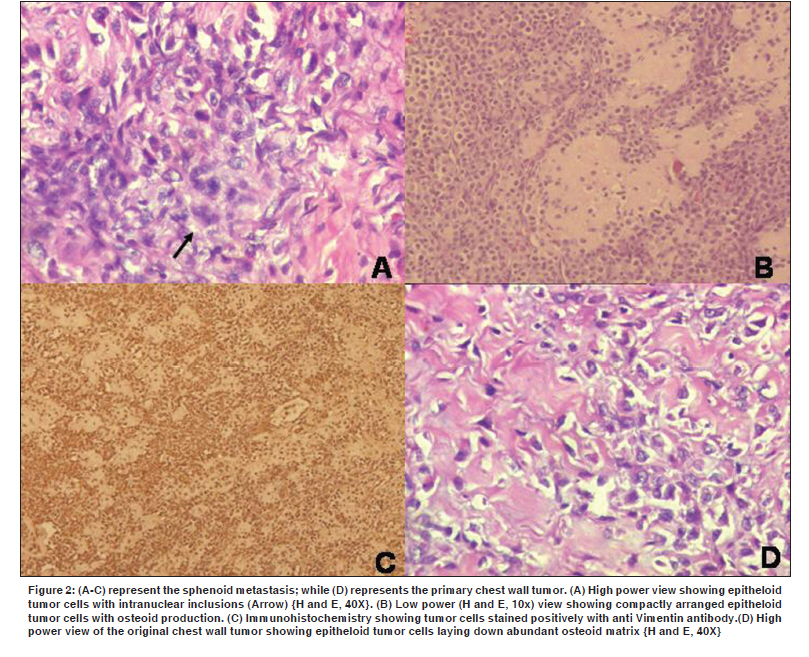
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 82-84 Letter To Editor Extraskeletal osteosarcoma of the chest-wall with delayed metastasis to the sphenoid Kelkar G, Moiyadi AV, Kane SV1 Neurosurgical Services, Department of Surgical Oncology, 1 Department of Pathology, Tata Memorial Hospital, Parel, Mumbai-12, India Code Number: cn10024 PMID: 20071803 DOI: 10.4103/0019-509X.58872 Sir, Extraskeletal osteogeosarcoma (ESOS) is a rare soft tissue tumor constituting 1.2% of soft tissue sarcomas (STS) and 5% of osteogenic sarcomas (OGS). [1],[2],[3],[4],[5] The histopathologic diagnosis of ESOS rests on the unequivocal demonstration of malignant sarcomatous elements producing osteoid tissue in a site not involving any host osseous elements (including peri- and parosteal involvement). ESOS arising from the chest wall is very rare, often associated with prior radiation. [6] Given the rarity of the occurrence of ESOS, little is known about its biological behavior. A 40-year-old man presented with a two-month history of watering of the left eye and blurring of vision. Fourteen years ago he had undergone wide excision and adjuvant radiation for a chest wall extraosseous mass. Histopathology had revealed high-grade sarcoma producing an osteoid and chondroid matrix. On examination he had reduced visual activity in the left eye (6/12 on Snellen's chart) with a temporal field defect. The MRI images [Figure - 1] showed a large expansile lytic lesion of heterogeneous intensity and moderate contrast enhancement, involving the greater wing of the sphenoid, extending into the adjacent intraorbital extraconal space producing optic nerve compression, as well as, into the temporal extradural space, lifting up the dura. The primary site of the surgery was normal. A whole body 2-deoxy-2(F-18)fluoro-D-glucose positron emission tomography (FDG-PET) scan showed increased FDG uptake in the left intraorbital lesion [SUV: 7.6] and no other active disease in the body. Fine needle aspiration cytology of the lesion was nondiagnostic. To resolve the diagnostic dilemma as well as relieve the optic nerve compression, the lesion was excised using a cranio-orbito-zygomatic approach. Postoperatively he had a dramatic recovery in his visual symptoms. The V/A in the left eye improved to 6/6 immediately. He subsequently had an uneventful recovery. Histology revealed an unequivocal sarcoma composed of epitheloid cells. Tumor cells revealed hyperchromatic nuclei with intranuclear inclusions [Figure - 2]A. Conspicuous osteoid production by tumor cells was seen [Figure - 2]B. Immunohistochemistry showed strong positivity for vimentin and focal positivity for the epithelial membrane antigen (EMA) [Figure - 2]C. Tumor cells were negative for cytokeratin, desmin, S-100, and CD-138. The Mib-1 proliferation index was 25%. The previous slides were reviewed and the histology was very similar [Figure - 2]D. Both revealed features of an osteoblastic type of ESOS. It was concluded that the sphenoid lesion was indeed a metastasis from the chest wall ESOS. The patient was advised chemotherapy, but he defaulted and presented again with periorbital swelling and an MRI suggestive of a local recurrence. He was subsequently given palliative radiotherapy [66Gy/ 33 # / 48 days], which he completed uneventfully. The swelling disappeared and at the last follow up, at six months, he was doing well. The biological behavior of ESOS is inadequately studied. Prognosis is poor even in patients who have received adequate therapy. The local recurrence rates are 26 - 69% and the five-year survival rate is 25 - 37%. [4],[5] The rate of metastasis of ESOS is 60%, [1],[2],[3],[4],[5] the commonest site being the lung. Metastasis to the sphenoid has not been reported. In general, metastases to the sphenoid are rare, with prostate being the commonest primary. [7] However, an osteosarcoma metastasizing to the sphenoid has not been reported to the best of our knowledge. Our case is probably the first report of an ESOS metastasizing to the sphenoid. The mean time of appearance of metastasis in an ESOS is very variable ranging from two months to 10 years.[4] Our patient had a delayed metastasis, almost 14 years later. We admit that the interval between the primary and secondary was very long. The other differential diagnosis entertained was a second primary osteosarcoma (OS). However, primary OS in the sphenoid, especially in the absence of prior radiation, is also very rare.[8] A majority of skull bone osteosarcomas are of the chondroblastic variety. In our patient both the tumors revealed identical features of an osteoblastic variety of OS. Monoclonality is impossible to prove. However, the weight of the circumstantial evidence favored a secondary from the previous ESOS. The role of surgery for metastases is controversial. In our patient surgery was indicated in order to resolve the diagnostic dilemma and to decompress the optic nerve, to salvage vision. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10024f2.jpg] [cn10024f1.jpg] |
| |||||||||

{kind=link}
{kind=link}