 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
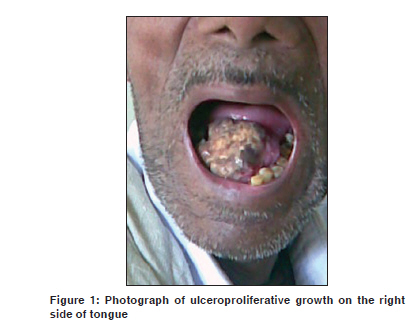
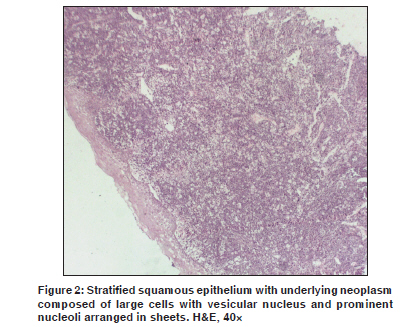
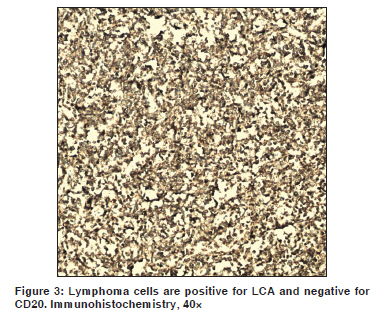
Indian Journal of Cancer, Vol. 47, No. 1, January-March, 2010, pp. 84-86 Letter To Editor Primary B cell non-Hodgkin's lymphoma of tongue Singh T, Amirtham U1 , Satheesh CT, Sajeevan KV, Jain A, Lakshmaiah KC, Babu KG, Lokanatha D Departments of Medical Oncology, 1 Pathology, Kidwai Memorial Institute of Oncology, Bangalore - 560 030, India Code Number: cn10025 PMID: 20071804 DOI: 10.4103/0019-509X.58873 Sir, The head and neck is the second most common region for extranodal lymphoma after gastrointestinal tract. [1] Waldeyer's ring lymphomas make up 50%-80% of the above and lingual tonsil lymphomas constitute about 3%-18%. [2] Only few cases of non-Hodgkin's lymphoma of the oral tongue have been reported in literature. [3],[4] Here, we report a case of oral tongue lymphoma diagnosed in our hospital. A 55-year-old man presented with a history of ulcer and slow painless growth on the right side of the tongue for 2 months [Figure - 1]. The patient was HIV positive since last one year and was not on any antiretroviral medications. On examination, he was pale, with upper cervical non-tender lymphadenopathy. Examination of oral cavity revealed ulceroproliferative growth of size 3×2×2 cm on the right anterolateral part of the tongue. Margins were indistinct and base of ulcer was necrotic, which was bleeding on touch. Hemogram revealed Hb of 9.4 g/dl, WBC of 6×10 9 /L (76%-N, 24%-L) and platelet count of 183×10 9 /L. Histopathological examination of the growth revealed poorly differentiated carcinoma [Figure - 2]. Fine-needle aspiration cytology of cervical lymphadenopathy was suggestive of reactive changes. Immunohistochemistry showed positivity for CD45 (LCA), CD138 and was negative for CD3, CD7, CD20, CD30 and CD68 [Figure - 3]. Findings were consistent with plasma blastic variant of diffuse large B cell lymphoma. Bone marrow aspiration, CSF examination and abdominal and thoracic CT scan revealed no involvement of other sites. IPI of the patient was 2/5 (Hb-9.4 and LDH 700U/L). HIV RNA levels were> 90,000 copies and CD4 count was 264/µL. Our patient was diagnosed with primary non-Hodgkin's lymphoma of diffuse large B cell type on the basis of immunohistochemistry and histopathological examination and his disease was staged as 1-E. He was treated with antiretroviral drugs and administered six cycles of 3 weekly CHOP. Following chemotherapy he received radiotherapy consisting of 50 Gy in 25 fractions over a period of 5 weeks by 6-Mv photon beam on a linear accelerator. He showed complete response after chemotherapy and radiotherapy. He was followed up for last 6 months without any disease recurrence and has been receiving antiretroviral drugs as per schedule. Others tumors that can be confused with lymphomas are melanomas, poorly differentiated squamous cell carcinomas, poorly differented adenocarcinomas, and are tumors such as neuroblastomas, rhabdomyosarcomas and Ewing's sarcomas. [5] Accurate diagnosis requires excisional biopsy of the extranodal mass. The most common symptoms are local swelling, pain and discomfort in the throat or ulceration. The tumor may manifest as a submucosal mass, a polypoidal bulky mass with a smooth mucosal surface or as an ulcerated lesion. Involvement of the intrinsic tongue musculature causes restriction of movement, dysarthria and dysphagia. Similar to lymphomas at other head and neck sites, oral lesions also seem to be quite sensitive to both radiotherapy and chemotherapy. Our patient was treated with chemotherapy and radiotherapy and had shown complete response to treatment and is disease free since then. In conclusion, though non-Hodgkin's lymphoma involving oral region is uncommon, it should always be considered in differential diagnosis of various benign and malignant lesions in this region because the treatment and prognosis for these conditions are quite different. A proper clinical evaluation, histopathologic as well as immunohistochemical evaluation of biopsy specimen may aid in the diagnosis, and thus help in management. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10025f3.jpg] [cn10025f1.jpg] [cn10025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}