 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 142-147 Original Article Quality of life among young women with breast cancer: Study from a tertiary cancer institute in south India Dubashi B, Vidhubala E, Cyriac S, Sagar TG Department of Medical Oncology, Cancer Institute (WIA), 18 Sardar Patel Road, Guindy, Chennai - 600 036, India Correspondence Address: Dr. Dubashi Biswajit, Department of Medical Oncology, Cancer Institute (WIA), 18 Sardar Patel Road, Guindy, Chennai - 600 036, India drbiswajitd@yahoo.com Code Number: cn10037 PMID: 20448376 DOI: 10.4103/0019-509X.63005 Abstract Background : The incidence of breast cancer in young patients less than 35 years is less than 1%. The physical and psychosocial morbidity may affect their ability to successfully function in their social roles. Hence we studied the quality of life (QOL) issues in this subset.Materials and Methods :Younger women with age less than 35 years, diagnosed with non-metastatic breast cancer at our Institute, from 1995 to 2005, were included in the study. Quality of life issues were studied during the follow-up using EORTC QOL C30 and BR23. Descriptive and inferential statistics were used in order to analyze the data. Results : A total of 51 patients were included for the study. The mean age at diagnosis was 30 years. The effect of breast cancer on the occupation and marital status was minimal. The global health status and the functional scores were high, while the overall sexual function was lower. The global health status was higher in the mastectomy group. The arm symptoms (P = 0.027) and pain were higher in the Breast conservation surgery (BCS) group. The sexual symptoms appeared to be higher in the ovary ablated group when compared to the ovary preserved group. The sexual functional scores (P = 0.02) and sexual enjoyment scores (P = 0.003) were better in the mastectomy group. Conclusion : The overall QOL in younger patients with breast cancer appeared to be good. The QOL and sexual function were marginally worse in the breast conservation group when compared to mastectomy group. Keywords: Quality of life, psycho-oncology, young breast cancer, breast conservation Introduction The diagnosis of breast cancer, despite improved overall survival, continues to generate fear and turmoil in the lives of women and their families. Prevalence studies of psychological distress indicate that one out of every three newly diagnosed patients experiences significant difficulty in adjustment. [1],[2],[3],[4],[5] Further evidence suggests that the diagnosis of breast cancer generates more anxiety than any other cancer diagnosis. [5] At the time of diagnosis patients experience uncertainty, confusion, and distress. Surgical options that include lumpectomy, mastectomy, and reconstruction present unique issues as the patient contemplates the advantages and disadvantages of each procedure. Following surgery, adjuvant therapy generates additional physiological assaults that further affect the body image, sexuality, and family life. [6],[7],[8] They require rehabilitative assistance beyond the physical domain. Major rehabilitation problems areas include physical, psychological, social, sexual, nutritional, financial, and vocational ones. [5],[6] For younger women the physical and psychosocial morbidity associated with the treatments may affect their ability to successfully function in social roles that typify this age group. Hence, we studied the QOL issues in this subset. The aims of the study were:
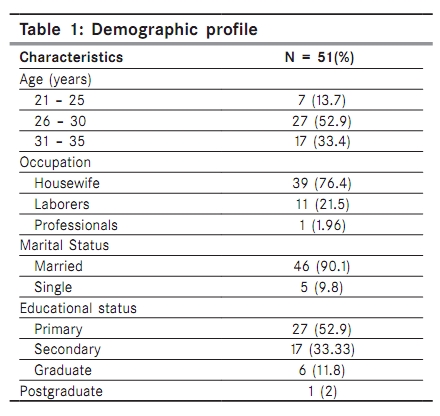
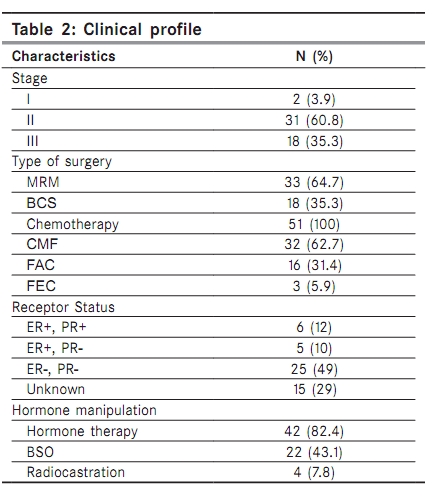
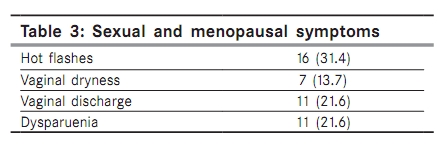
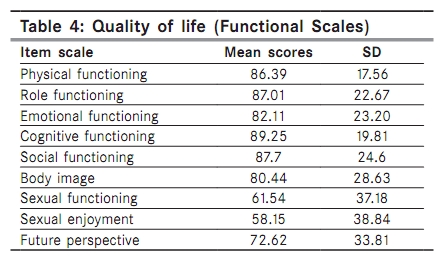
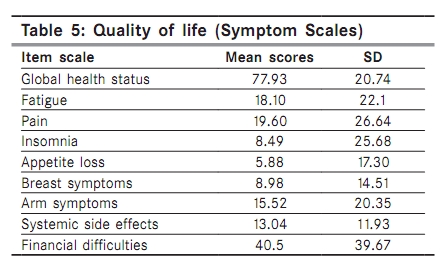
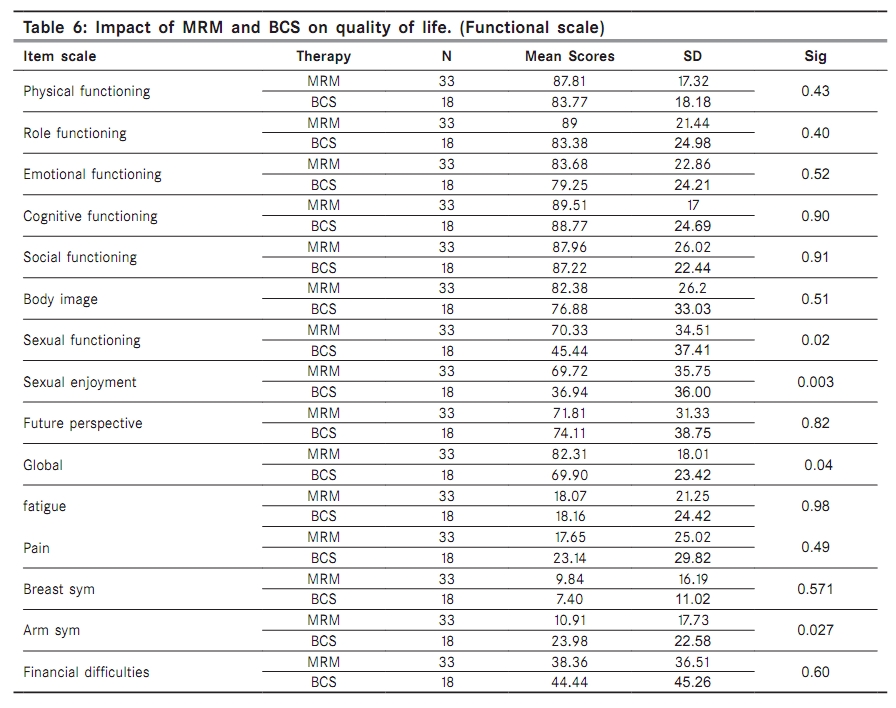
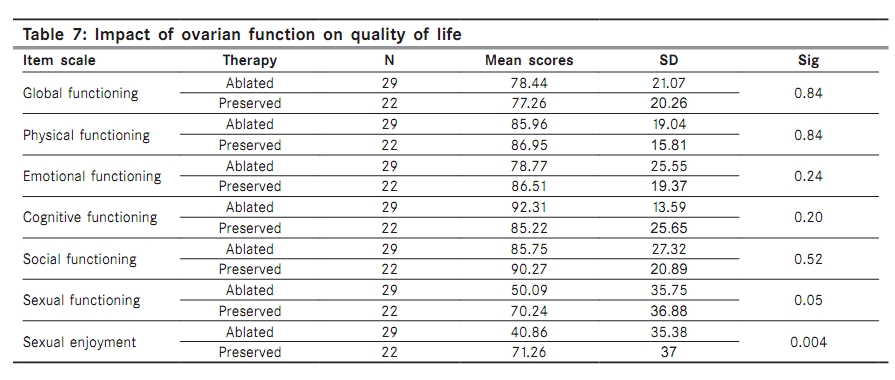
Materials and Methods Younger women diagnosed with breast cancer, who underwent protocol treatment from 1994 to 2005 at our Institute, which is a tertiary care cancer center, were included for the study. Patients with age less than or equal to 35 years with TNM stage I, II, and III, and those who had completed a minimum of 18 months follow-up were included in the study. Any patient with metastasis and histological diagnosis of sarcoma and lymphoma was excluded. The medical records of 100 patients who met the inclusion criteria from 1994 to 2005 were reviewed and included in the study. The women were then contacted by phone or letter and were asked to come for a review to the breast cancer clinic, where the QOL questionnaire was administered, after taking informed consent. Depending on the stage of the disease, the patients either underwent initial surgery or neoadjuvant chemoradiotherapy followed by surgery. [9] All patients received hormonal therapy irrespective of the receptor status. Ovarian ablation was offered to all the patients. Sociodemographic variables included age at diagnosis, marital status, level of education, and employment status. Medical variables included cancer stage, type of surgery, hormonal status, menopausal status, ovarian function, and child birth after diagnosis. The QOL issues were studied using the EORTC module QLQ - C30 and the BR 23 Questionnaire. The questionnaire had been validated on Indian patients. [10] The EORTC module QLQ C 30 is a 30 item questionnaire composed of five multi-item functional subscales: Physical health, role function, emotional function, cognitive function and social function; three multi-item symptom scales measuring fatigue, pain, and emesis; a global health subscale and six items to assess the financial impact and general symptoms. The BR-23 module evaluates the treatment-related symptoms of breast cancer. It incorporates three functional scales (body image, future perspectives, and sexuality) and four symptom scales (arm symptoms, breast symptoms, hair loss, and side effects) of systemic therapy. In addition to this, a few other issues related to fear of recurrence and partner response, sexual dysfunction, and menopausal symptoms were also assessed The BR-23 module evaluates the treatment-related symptoms of breast cancer. In addition to this, a few other issues related to sexual dysfunction and menopausal symptoms were also assessed. The questionnaires were available in four languages namely English, Tamil, Telugu, and Malayalam, which were administered according to the patient′s vernacular language. The patients completed their questionnaire on their own; however, some of them required assistance. The study was cleared by the institute′s Ethical Board. Scoring of the QLQ - C30 and BR-23 was done according to the procedures described in the European Organization for Research and Treatment of Cancer (EORTC) manual. Descriptive and inferential statistics were used in order to analyze the data using SPSS version 13. Results A total of 51 patients who attended the breast clinic and completed the questionnaire were taken up for the study. The mean age at diagnosis was 30 years. The mean age at the time of QOL analysis was 35 years. The demographic profile of the study population is as follows: [Table - 1]. Twenty-seven (52.9%) patients had completed primary education. Two patients who were housewives at diagnosis took up jobs as laborers after the diagnosis of cancer. One laborer and the other a professional left their jobs and became house wives. Of the 48 patients who were married, two got divorced, and two of them became widows during the course of the treatment. Of the five who were single at diagnosis, four got married and one continued to be single. Family history of cancer was present in six patients (11.8%). Thirty-one (60.8%) patients were in stage 2. All the patients underwent surgery with 35% of the patients receiving BCS. Forty-nine percent of the patients were receptor negative. Bilateral salpingo-oopherectomy was done in 43.1% of the patients, while radiocastration was performed in 7.8% of the patients; 49.1% of the patients did not give consent for ovarian ablation. Nine patients (17.6%) had chemotherapy-induced amenorrhea of which three had permanent ovarian failure. Hormonal therapy with tamoxifen was administered to 82.4% of the patients. The clinical profile is summarized in [Table - 2]. Twenty-two (43.1%) patients had intact menstrual function, of which two patients had irregular cycles. Premature menopause was seen in 29 patients. Of the nine patients with chemotherapy-induced amenorrhea, three patients had permanent ovarian dysfunction. Three patients had successful pregnancy after completion of therapy [Table - 3]. The EORTC QLQ C30 and BR23 questionnaires were used for the assessment of the QOL. The mean global health status score was 77.93. The functional scores of the roles, physical, emotional, cognitive, and social, and body image, were high ranging from 80 to 89.The functional scores of sexual function, sexual enjoyment, and future perspective were low, in the range of 58 to72 [Table - 4] and [Table - 5]. The symptom scales of fatigue, pain, insomnia, loss of appetite, breast, arm, and systemic side effects were low; in the range of 5 to 20. Only the financial score of the symptom scale was high with a score of 40.5 . Sexual functioning and sexual enjoyment were significantly better in the mastectomy group when compared to the breast conservation group. All other functional scales like physical health, role function, emotional function, cognitive function, social functioning, and body image were similar in both the groups [Table - 6]. The global health status (P = 0.04) was better in the mastectomy group when compared to the breast conservation group. The arm symptoms were statistically higher in the breast conservation group (P = 0.027). Local pain was found to be slightly higher for the BCS group. The financial problems were also more in the BCS group. The fear of recurrence was higher in the mastectomy group. With respect to their partners, patients with BCS had higher partner neglect (28%) and were also overprotected (28%) more than the MRM group. The sexual functioning and enjoyment were better in the ovary preserved group rather than in the ovary ablated group, and it was statistically significant. The emotional, social, body image, and future perspective appeared to be better in the ovary preserved group, although did not reach statistical significance. The overall global health status appeared to be similar in both the groups [Table - 7]. The mean duration of follow-up was 5.33 years (2 - 11 years). The emotional and body image scores were slightly less in those with more than six years of follow-up, when compared with those who had less than or equal to five years of follow-up. The global QOL and other functional and symptom scales were similar in both the groups. Discussion The incidence of breast cancer in the age group of 20 to 29 years is less than 1%, and it is 6.5% in the age group of 30 to 39 years. [1],[2],[3] These patients are in the reproductive age group and are concerned with fertility issues. The overall QOL was comparable, with exception to sexual functioning, which was lower when compared to a study conducted in Indian women with breast cancer, by Parmar et al.[10] As found in other studies, sexual problems in younger women were not related to the sociodemographic factors or type of breast cancer surgery. [11] The QOL and sexual function were marginally worse in the breast conserved group when compared to mastectomy. The impact of the QOL on the two treatment groups, namely breast conservation and mastectomy, are gross categories that fail to distinguish the variety of procedures and the adjuvant treatment like chemotherapy, radiotherapy, and hormonal therapy. There are several confounding factors. The reason for the overall QOL being poorer in the BCS group is that the arm symptoms and the pain are not dependent on whether the breast is conserved or not. In our study the arm symptoms were significantly (P = 0.027) higher in the breast conserved group. It has been seen in various studies that with increasing time the QOL among the different groups becomes less obvious. [12],[13],[14] Our study again was of patients who were long-term disease-free survivors. Breast conservation surgery did not improve the body image score in our study. The impact of BCS and MRM on the QOL has shown contradictory results in different studies. A study by Janni et al., showed that no difference was observed in the QOL, which was administered 46 months following primary treatment, between the two groups. [15] In contrast Cohen et al. found that women who had BCS experienced significantly greater psychological distress and marginally worse QOL 40 months after surgery. [16] The patients with ovarian ablation had slightly more sexual symptoms than the ovary preserved group. Stephanie in her study on sexual problems after surgery found that the sexual problems in younger women were not related to sociodemographic factors or type of breast cancer surgery. [17] The fear of recurrence appeared to be higher in the mastectomy group in our study. The reason could be that patients felt that mastectomy was done for advanced disease and hence there was a higher chance of relapse. This was investigated in eight studies. Only two studies favored the mastectomy group. [18],[19] The financial constraints also appeared to be higher for the BCS group. This could be attributed to the length and costs of breast conserving treatment, with subsequent follow-ups and screening mammograms being higher in this group. [18] In our study chemotherapy-induced amenorrhea was seen in 17.6% of the patients; 11.6% of the patients had temporary amenorrhea, and 6% had permanent amenorrhea. In the review by Bonnie et al., of the 128 patients, 59% continued to menstruate, 32% experienced temporary amenorrhea, and 9% experienced permanent amenorrhea. [20] Three patients had successful pregnancies following completion of surgery. There are wide variety of procedures and applied assessment instruments for measuring the QOL making it difficult for studies to be compared. Hence more studies in this subset of patients, in the near future, may throw some light on them. Conclusion This study includes very young breast cancer survivors, less than 35 years of age, where the biology of the disease, QOL, and fertility issues are unique. The effect of breast cancer on the occupation and marital status appears to be minimal. The overall QOL with the exception of sexual function appears to be good. The QOL and sexual function are marginally worse in the breast conservation group when compared to the mastectomy group. Preparing younger women for the impact of breast cancer and helping them deal with problems may improve their QOL. Younger breast cancer survivors may be in need of interventions that specifically target these issues, such as non-systemic products, to alleviate vaginal dryness and also programs to help women deal with body image concerns. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10037t3.jpg] [cn10037t7.jpg] [cn10037t5.jpg] [cn10037t4.jpg] [cn10037t2.jpg] [cn10037t6.jpg] [cn10037t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}