 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
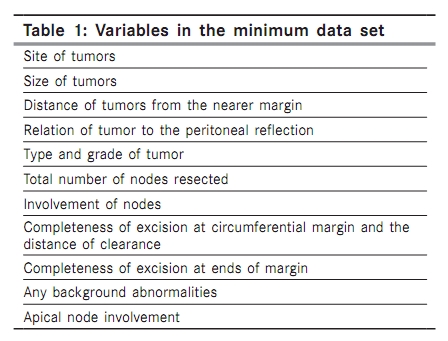
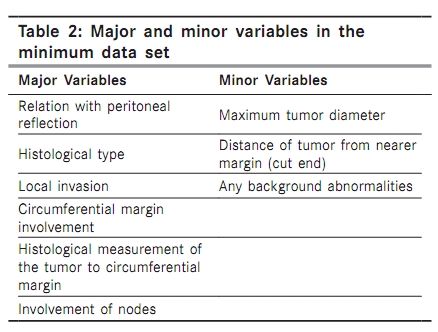
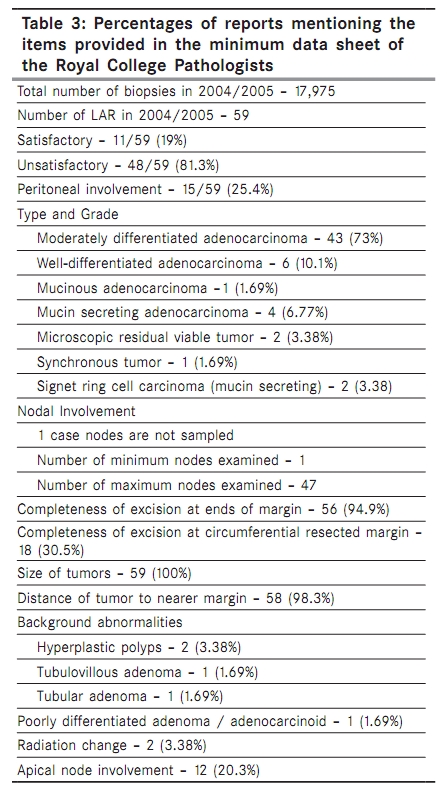
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 156-159 Original Article Completeness of low anterior resection pathology report: A hospital-based audit with recommendations on improving reporting Nambiar A, Vivek N, Bindu MR, Sudheer OV1 , Bai L Departments of Pathology and 1 Gastrosurgery, Amrita Institute of Medical Sciences, Elamakara, Kochi, India Correspondence Address: Dr. Ajit Nambiar, Department of Pathology, Amrita Institute of Medical Sciences, Elamakara, Kochi, India nambiarajit@yahoo.com Code Number: cn10040 PMID: 20448379 DOI: 10.4103/0019-509X.63010 Abstract Aims: To audit the information content of the pathology report on Low Anterior Resection (LAR) specimens and to provide recommendations in order to improve the existing standard of reporting.Materials and Methods : All the reports of LAR specimens during 2004 - 2005 were collected from the Hospital Information System (HIS). Individual items of information were compared with the minimum data sets provided by the Royal College of Pathologists (RCP). Results : Fifty-nine reports were audited. Nineteen percent of the reports were classified as satisfactory. Although many items were well reported, only 30.5% (18/59) of the reports contained a statement on the completeness of excision at the circumferential resected margin and only 25.4% of all reports mentioned the relation of tumors to the peritoneal reflection. Conclusion : The information content of the reports on colorectal cancer resection specimens is inadequate. The use of the standard proforma (template) for reporting rectal cancer is therefore recommended, along with improved education, review of laboratory practices in the light of current knowledge, and further motivation of pathologists through their involvement in multidisciplinary cancer management. Keywords: Audit pathology report Introduction Histopathology reporting of resection specimens for colorectal cancer provides important information for the clinical management of patients as well as for the evaluation of health care. Quality pathology reporting provides robust information for cancer registry, for clinical audits, and for ensuring comparability of patient groups in clinical trials. It is therefore very important for pathology reporting to be very accurate. Several guidelines on reporting of resection specimens in colorectal cancers have been published in various standard text books of pathology, [1],[2] by various expert working groups. [3],[4],[5] The recommendations have been varied from a detailed description of reports to the minimum requirements, whose relevance to current patient management attempts to be more evidence based. In rectal cancer, there is evidence that involvement of the circumferential resection margin is an important predictor of local recurrence and patient survival, [6] and might identify patients who benefit from postoperative adjuvant therapy. [7] To the best of our knowledge, there is no published information on the quality of rectal cancer reporting in the current histopathology practice, in India. In this study we present the finding on a hospital-based audit of a pathology report, on low anterior resection specimens. Materials and Methods All reports on low anterior resection in the Pathology Department, during 2004 - 2005 were retrieved from the Hospital Information System (HIS). All the data were compared with the minimum data set by the Royal College of Pathologists, for the presence or absence of each variable in the final histopathology report. The variables in the minimum data set are shown in [Table - 1]. The variables were classified as major or minor, depending on the impact of the variable on the prognosis and the impact of the omission on treatment planning [Table - 2]. The reports were further classified as satisfactory if no major omission, with a permissible one or two minor omissions, were noted. A strict criteria was imposed with regard to unsatisfactory reports. The report was considered unsatisfactory even when one of the major variables was not mentioned. This audit was done independently by a surgical pathology trainee in the department. All the data retrieved were analyzed and results were finalized on the data sheet provided. Results There were 17,975 biopsy specimens received in the department during 2004 - 2005. In total, 59 reports were available for assessment. The percentage of reports mentioning statements on each of the individual items of information compared with the minimum data set by the Royal College of Pathologists is shown in [Table - 3]. A statement on the completeness of the excision at the ends of the margin was given in 94.9% of the reports. Only 25.4% mentioned the tumors above or below the peritoneal reflection. Completeness of excision at the circumferential resected margin was poorly reported and distance of clearance was mentioned in 8.47% of the reports. All reports mentioned the histological type of the tumors, grade and staging, and involvement of the regional lymph nodes. Almost all reports described the distance of the tumors to the nearer cut margin (98.3%). The statement of the involvement of apical nodes is described only in 20.3%. Background abnormalities were present in 11.8% of the reports. Discussion Audit is a systematic and independent examination to determine whether quality activities and related results comply with the planned arrangements, and whether these arrangements are implemented effectively and are suitable to achieve the objectives. [8] Local audit systems are concerned with aspects of daily work in the department and are essentially aimed at feedback on the performance. It is imperative that such systems should come from within a department, rather than be imposed from outside. Various aspects of work - description of the whole specimen, microscopic report, turnaround time, laboratory performance or secretarial performance can be audited. We audited only the information content of the issued low anterior resection specimens for colorectal cancers. We have not assessed the diagnostic precision, sampling of specimen for microscopic examination or the accuracy of any data, although these factors will obviously influence the quality of the information provided. We have assessed only the completeness of the final report with regard to a defined number of items of information. The audit has been done by an independent surgical pathology trainee in an unbiased manner. The most important deficiencies relate to a poor description of the circumferential resection plane involvement in rectal carcinomas and the number of lymph nodes involved by metastasis. The circumferential margin involvement in rectal cancer is an important prognostic indicator, having high predictive values for both survival and local recurrence. [6],[9] It also influences the decision on whether to use adjuvant radiotherapy or chemotherapy. Our finding that this information was given in only 30.5% of the cases, suggests that effective patient treatment may have been compromised by incomplete pathological reporting. Involvement of the lymph node is another factor that is used to select patients for postoperative chemotherapy. [10] Keeping stringent criteria for categorization of a report we found that only 19% of our reports were satisfactory. A regional audit from Wales, on colorectal pathology reporting, showed that 46.6% of the rectal cancer reports were complete. [11] The circumferential margins in the worst performing laboratory, in the regional Wales audit, were reported in 8.3% of the cases, while they were reported in 78.1% of the best performing laboratories, with a value of 51.6% for Wales as a whole. [11] Audits on histopathology reporting of cancer resection specimens show that the consistency of reporting essential data items leaves much to be desired. Reasons may be a lack of resources, lack of incentives, and discontentment with the standards that have been set or even pure apathy. However, the most important is perhaps an inadvertent omission of occasional data items by pathologists who are otherwise diligent in their reporting. This may be the result of the lack of a formal reporting process and the most appropriate solution in the use of the template proformas along with guidelines for the reporting of common specimens. The Sheffield study on the effect of four different interventions on the reporting of colorectal cancer showed that only when template proformas were introduced did the data completion rates reach 100%. [12] These templates of the minimum data items agreed upon should be integrated into departmental computerized information and reporting systems. The CROPS (Cancer Registration through Online Pathology Systems) project in Wales, performed as a randomized controlled trial of implementing such computer proforma reporting of breast and colorectal cancer specimens showed a 24 - 28% improvement in the completeness of minimum data items. [13] One of the commonest criticisms of template proforma reporting is removing the element of subjectivity, which is an essential armory in an individual pathologist′s hand. However, on the other hand the clinicians are very enthusiastic and happy about the consistent format of the reports produced. A need for change in the mindset of the pathologists is essential. Even examinations must add completion-oriented reporting to conventional diagnosis-oriented systems. Pathologists must be active in tumor boards and their role in patient management needs must be continually reinforced. There is a need to emphasize this in pathology training programs, with the ultimate aim of improving the quality standards of service delivery and laboratory accreditation. We believe that continuing medical education toward informing pathologists of newer approaches to dissecting and sampling resection specimens will maximize the report output in an efficient manner and also help in highlighting how clinical decisions on adjuvant therapy depend more than ever on careful pathological staging and evaluation of resection margins. The department heads and seniors should ensure that the histopathology section has the resources to examine and report the specimens to high standards and to maintain their standards through an internal audit. The onus is perhaps also on the surgeons and their oncologist colleagues to see to that the pathologists are seen as key members of the multidisciplinary team that delivers effective cancer care. The need for lead pathologists, for site-specific cancers, within the hospital set up, will go a long way in providing better services. An audit in a hospital-based practice is to be viewed not only as a performance or completeness of the report assessor, but also to introspect the weakness and to correct the deficiencies. No audit has any meaning if the conclusion and recommendations are not taken to their meaningful ends. The ′closing of the circle′ is an important aspect of the audit exercise. A constant review of laboratory practices in light of current knowledge is also essential. Improving the quality and completeness of the information provided not only aids patient management, but also benefits the pathologist′s input into the audit, clinical trial, and cancer registry. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10040t1.jpg] [cn10040t3.jpg] [cn10040t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}