 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
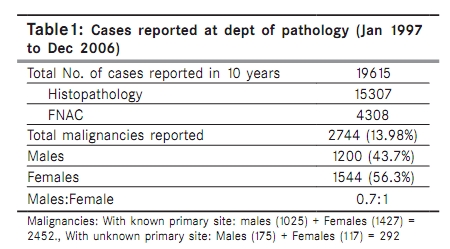
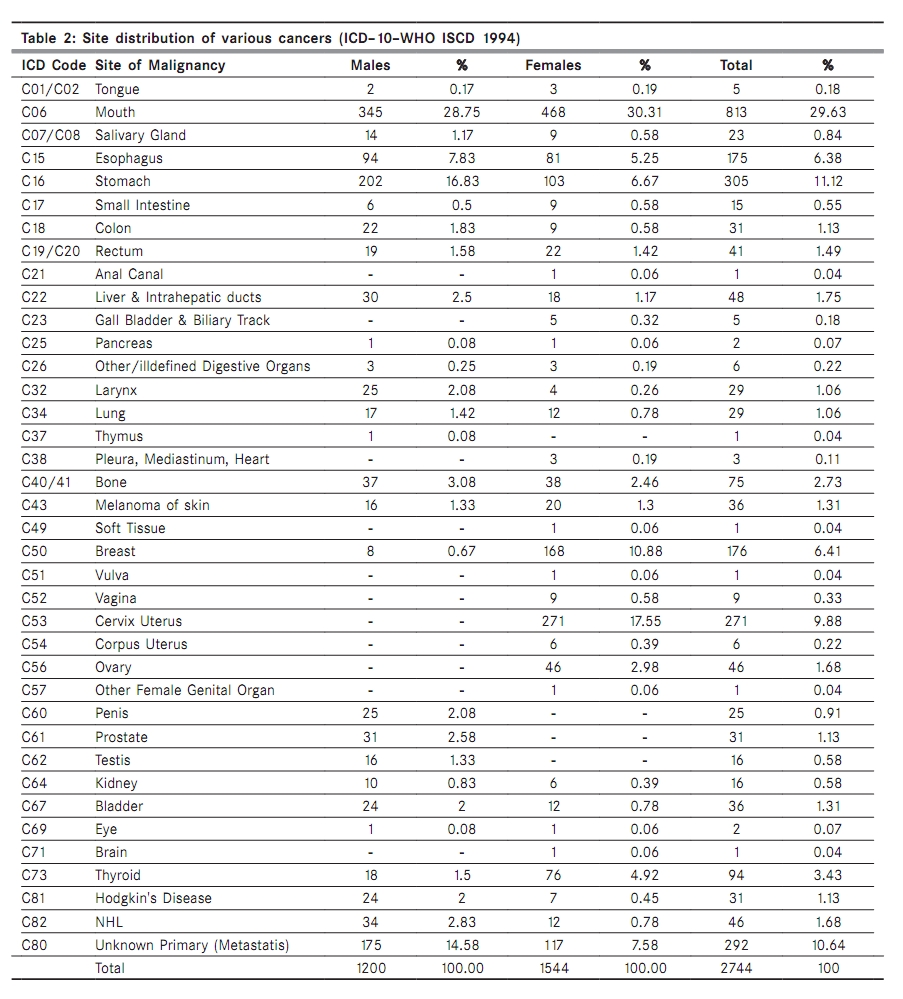
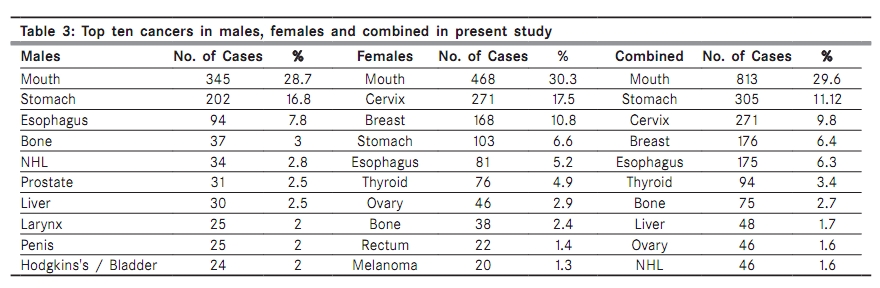
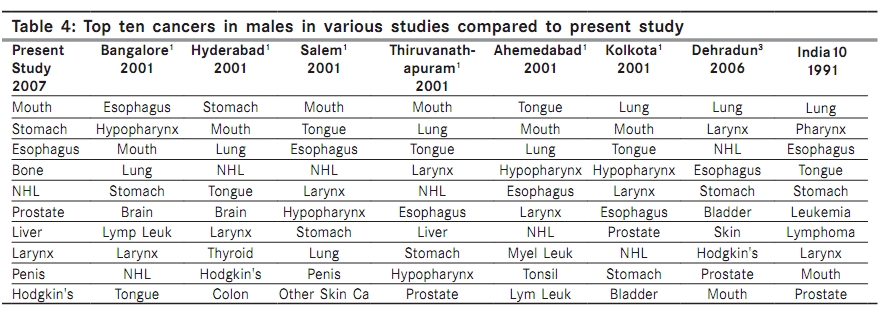
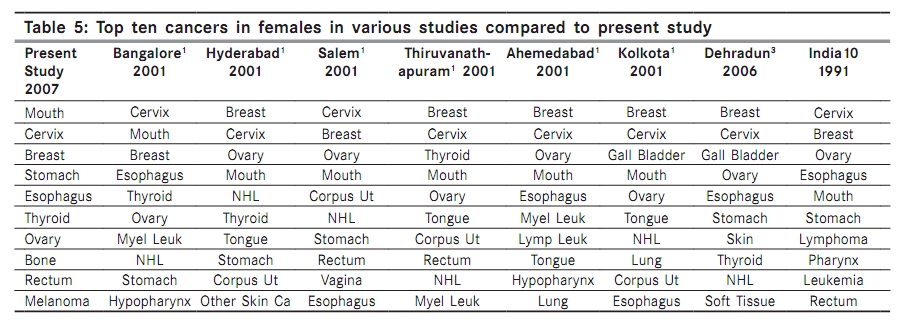
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 160-165 Original Article Cancer profile in Kolar: A ten years study Kalyani R, Das S, Bindra Singh MS, Kumar HML Department of Pathology, Sri Devaraj Urs Medical College, Sri Devaraj Urs University, Kolar, India Correspondence Address: Dr. Kalyani R, Department of Pathology, Sri Devaraj Urs Medical College, Sri Devaraj Urs University, Kolar, India drkalyanir@rediffmail.com Code Number: cn10041 PMID: 20448380 DOI: 10.4103/0019-509X.63011 Abstract Context: Cancer profile varies in different regions and depends on race, lifestyle and diet. The study of a cancer profile helps to know the common cancers in a particular population, its probable risk factors and also helps in cancer control programs.AIM: To study the cancer profile at Kolar, based on Pathology Department records. Settings and Design: Retrospective study from January 1997 to December 2006. Materials and Methods: Cancer cases diagnosed by fine needle aspiration cytology (FNAC) and histopathology in the Department of Pathology were included in the study. The relevant history, clinical findings, and sociodemographic information of each case was retrieved from hospital records. Statistical Analysis Used: Descriptive statistics. Results: Out of a total of 19,615 cases reported at the Department of Pathology, 2,744 (13.98%) were cancer cases. The peak incidence was in the fifth decade in females and the seventh decade in males. Male : Female ratio was 0.7 : 1. Overall there was a steady rise in the number of cases from year 1997 to 2006. The top ten cancers in males were of oral cavity, stomach, esophagus, bone, non-Hodgkin's lymphoma (NHL), prostate, liver, larynx, penis, and Hodgkin's disease / bladder and those in females were oral cavity, cervix, breast, stomach, esophagus, thyroid, ovary, bone, rectum, and melanoma. Conclusions: Oral cavity and upper gastrointestinal cancers predominated in both genders. In females, cervical cancer predominated over breast cancer. Thyroid cancers were relatively more common in this region especially in females. Keywords: Cancer, profile, Kolar Introduction Cancer is the most dreaded disease in the world. The incidence of cancer is increasing with each year and it is attributed to the changes in lifestyle and increase in life expectancy. [1],[2],[3] The cancer profile varies in different parts of the world and an epidemiological study helps to know the common cancers prevalent in particular segments of a population and the risk factors involved. [2],[3] However, there is lack of definitive information regarding hospital-based cancer profile in Karnataka. The present study was undertaken atKolar, which is located in southeastern Karnataka. Materials and Methods A 10-year hospital registry-based retrospective study from January 1997 to December 2006 was undertaken in the Department of Pathology attached to a 750 bedded teaching hospital, located in Kolar, which serve as a tertiary health. It catered mainly to the rural population, as also to the people of Kolar town and the neighbouring districts of the adjacent states. A majority of patients who used the hospital services were agriculturists and labourers by occupation. The population of Kolar district is 2,523,406, population density is 307 / sq.km, and females are 970 / 1000 males. [1] The literacy rate is 73.14% in males and 52.81% in females. [1] The Kolar district shares the borders of Andhra Pradesh and Tamil Nadu, which has influenced the food habits and lifestyle of the people. Rice and ragi are the staple food. The food is very spicy and there is increased use of tobacco and alcohol in both sexes, especially in lower socioeconomic group. As this region is a dry place, people depend on deep bore well water for drinking purposes. All cancer cases reported in the Department of Pathology by histopathology and fine needle aspiration cytology (FNAC) were included in this study. Multiple specimens of a patient, especially where FNAC was followed by histopathology, were considered as one case. Only those FNAC cases that were not followed by a histopathological study were counted separately. All hematological malignancies were excluded. The information of each case regarding age, sex, occupation, residential area, food habits, use of alcohol and tobacco, history of exposure to risk factors, type of drinking water (bore well / tap water), date of admission, clinical diagnosis, and final diagnosis were retrieved from hospital records. Fifty cases lacking relevant information like age, occupation, and adequate investigation were excluded. The diagnosis of each case was revised and confirmed by three pathologists (KR, HK, SD). Any diagnostic discrepancies were confirmed by special stains. The cumulative data was then categorized and coded according to the International Classification of Diseases (ICD 10), World Health Organization (WHO) and International Society for Clinical Densitometry (ISCD) 1994. [1] The metastatic cancers of unknown primary were grouped separately. Descriptive statistical analyses were done. The cases were grouped according to age, sex, year-wise, and top ten common cancers. These findings were compared with similar studies. The clinical follow-up of the cases was not considered. Ethical clearance for conducting the study was obtained from the Ethical Clearance Committee of the institute. Results Among 19,615 cases of histopathology and FNAC reported, a total of 2744 (13.98%) were malignant, of which 1200 were males and 1544 females, with male : female ratio of 0.7 : 1, indicating female preponderance. Of the total malignant cases 292 cases were metastatic cancers of unknown primary site [Table - 1]. Among all the cancers, cancer of the oral cavity was the leading cancer in both sexes (total n = 814 cases). In lymph node malignancies (n = 369 cases), metastatic cancers outnumbered (n = 292 cases) Hodgkin′s disease and NHL (total n = 77) in both sexes [Table - 2]. The maximum cases were in the age group of 60-69 years. Among males, the maximum cases were in the age group of 60-69 years (n = 333) and in females 40-49 years (n = 415). Males predominated in age groups of 10-19 years and 60-89 years, whereas, females in age groups of 20-59 years (reproductive age) and 90-99 years. Male and female cases were equal between 00-09 years. However, the frequency of malignancies reduced toward the extremes of age in both the genders. Considering the distribution of cancers year-wise, overall there is a steady rise in the number cancers from the year 1997 to 2006. Cancer of oral cavity predominated in both genders. The top ten sites most frequently involved by cancer in males were oral cavity, stomach, esophagus, bone, NHL, prostate, liver, larynx, penis, and Hodgkin′s disease / bladder cancer, whereas, the sites in females were oral cavity, cervix, breast, stomach, esophagus, thyroid, ovary, bone, rectum, and melanoma skin [Table - 3]. From the hospital records it was observed that a majority of the patients from both genders, especially those cases of oral cancers, had a habit of tobacco chewing and use of alcohol. However the risk factors are not analyzed in this study. Discussion The incidence and cancer profile varies in developed and developing countries. Incidence is high in developed countries because of the affluent society, diet, and lifestyle. [2],[4] Twenty-five percent of cancer in developing countries are also associated with chronic infection. Increasing life expectancy is one important factor for the increased incidence of cancer. [2] Globally life expectancy at birth has increased from 45 years in 1950 to 66 in 2000 and is expected to reach about 77 years in 2050. [2] Life expectancy at birth in India, reported for 2005, is 62 years in males and 64 years in females. [4] However, genetic susceptibilities may significantly alter the risk from environmental exposure. The incidence of cancer in this study was 13.98%, which was comparable to other studies. [3],[5],[6],[7] Cancer is predominantly a disease of middle and old age. The peak age of occurrence of cancer in this study was the seventh decade in males and fifth decade in females, comparable to most of the studies except Bankura′s, where it is fifth decade in males and fifth / sixth decade in females. [3],[5],[6],[8],[9] In this study the male female ratio was 0.7:1, showing a female preponderance, which was compared with other studies. [3],[5],[6],[7],[8],[10] Gender difference depends on exposure to causative agents and not due to susceptibility of any sex. [4] In the present study the commonest site of cancer was the oral cavity, which predominated in both genders (n = 814) and histologically almost all were squamous cell carcinoma. Such a high prevalence is also seen in Salem, Thiruvanthapuram, Ahmedabad, Ludhiana, Western Rajasthan, and other South Central Asian countries, that is predominantly in the developing countries where there is an increased use of tobacco and alcohol [Table - 4] and [Table - 5]. [1],[2],[6],[9] The habit of reverse smoking, especially chutta, oral snuff, betel quid, or pan with tobacco, along with alcohol, is more common in this region of the present study, especially in the lower socioeconomic class, in both genders. Human papillomavirus (HPV) is also a factor causing cancer of the oral . It is estimated that women with a history of in-situ or invasive cervical cancer has 2.4 times the increased risk of oral / laryngeal cancer. [2] Detection of precancerous lesions or use of oral cytology with toluidine blue helps in the early detection of cancer. [2] In females cervical cancer is more common (n = 271) compared to breast cancer and histologically a majority were squamous cell carcinoma (n = 262) followed by adenocarcinoma (n = 12). It occupies second place after cancer of oral cavity in the present study. Studies in Hyderabad, Thiruvanthapuram, Ahamedabad, Kolkata, Dehradun, and Western Rajasthan showed similar high incidences [Table - 5]. [1],[3],[9] Carcinoma cervix is more common in developing countries. Early marriage, age of first pregnancy, multiple pregnancies, decreased genital hygiene, and sexual , influence cancer of the cervix, which also been observed in the present study. [6],[9],[10] Penile hygiene of male partner is also an important factor. [2] HPV is well associated with carcinoma of the cervix. WHO has recommended screening of every woman between 35 and 40 years of age. [9] Regular screening programs and Pap smears help in the early detection of carcinoma of the cervix. [2] Breast cancer is the next common cancer in females (n = 168) in the present study and histologically a majority were infiltrating ductal carcinoma (n = 159) followed by medullary carcinoma (n = 8). However, studies in Ludhiana, Dehradun, Eastern Rajasthan, and Srinagar showed increased incidence than cervical cancer. [3],[6],[7],[8] Breast cancer is common in affluent societies having a western lifestyle. [8],[10] Male breast cancer is 100 times less frequent than female breast cancer. [2] We had eight male breast cancers in the present study. Population-based screening, especially mammography, has decreased the mortality by 25 30%. [2] Females with a family history of breast cancer should an intensive screening program. [9] Stomach cancer is the second most common in males (n = 202) and fourth most common in females (n = 103), in the present study, and histologically a majority were adenocarcinoma (n = 293) followed by squamous cell carcinoma (n = 5). It forms 60% of the total cancer in developing countries with male preponderance. [2] Studies in Hyderabad, Srinagar, and Dehradun also showed increased incidence. [1],[3],[7] Cancer of stomach is one among the top cancers in South Karnataka and the South Indian states where rice is the staple food. [1],[2] In the region of the present study rice is staple food, also food is very spicy, with increased use of tobacco and alcohol. Increased intake of salt, preserved food, smoked food, smoking, and carbohydrate-rich diet are associated with increased incidence. [2] Salted and smoked foods increase nitrates, decrease antioxidants, and cause gastric atrophy. [2],[7] A carbohydrate-rich diet is usually associated with decreased protective micronutrients such as Vitamin C, Vitamin E, and tocopheral, which increase the risk of stomach cancer. [2] Intake of refrigerated food decreases the risk of carcinoma of the stomach. [2] Onions and fresh vegetables / fruits have high antioxidants and have decreased risk of stomach cancers. [2] However, a study at Ludhiana has showed decreased incidence of stomach cancer in Punjabis, which is attributed to their increased intake of milk, milk products, and wheat floor. [6] H. pylori infection contributes to 40-70% of stomach cancer. [2] Esophageal cancer is next common cancer in this study in males (n = 94) and females (n = 81) and histologically, a majority were squamous cell carcinoma (n = 166) followed by adenocarcinoma (n = 8). It is the common cancer as shown in various studies in Bangalore, many districts of South Karnataka, Salem, Thiruvanthapuram, Ahmedabad, Kolkota, Dehradun, Srinagar, Ludhiana, and Eastern Rajasthan. [1],[3],[6],[7],[8],[10] Eighty percent of esophageal cancer in developing countries is squamous cell carcinoma and associated with smoking, alcohol, malnutrition, use of hot beverages, betel nut chewing, along with decreased intake of fresh fruits and vegetables. [2] Most of the cancers in developed countries are adenocarcinomas, seen commonly in white men, associated with obesity and chronic gastroesophageal reflux. [2] Esophageal cancer is also related to the intake of tanin in various forms, agemonse seeds, as also infection by HPV and Fungi. [6] In the present study a majority of esophageal cancers were squamous cell carcinoma, which could be attributed to an increase in the use of alcohol and tobacco. Bone cancer constituted 37 cases in males and 38 in females. The majority were osteosarcoma. Ionizing radiation and viruses are the associated etiological factors in bone cancer. [9] NHL and Hodgkin′s disease is more common in males (n = 34 and 24, respectively) than females in this study. NHL is more common in developed countries. [2] Hodgkin′s disease in developing countries is seen more in children and elderly people, whereas, in developed countries it is common in young adults. [2] Virus is associated as one of the etiological factors in the pathogenesis of lymphoma. [2] Thyroid cancers are relatively common in this region and are more common in females (n = 76) than males (n = 18) and histologically, a majority were papillary carcinoma (n = 83) followed by medullary carcinoma (n = 7). Thyroid cancer forms one among the top ten cancers in the studies at Bangalore, districts of South Karnataka, Hyderabad, Thiruvanthapuram, Dehradun, and Eastern Rajasthan. [1],[3],[8] It can be attributed to bore well water, ionizing radiation, cruciferous and goitrogenic vegetables. [2] It is reported that too much iodine causes papillary carcinoma and iodine deficiency causes follicular carcinoma. [2] Cancers of male reproductive organs especially prostate cancer (n = 31) and penile cancer (n = 25) also occupy a place among the top ten cancers in this study. Prostate cancers are common in developed countries with high calorie diet, physical inactivity, black men, and it is common in old age. [2],[3] Life time risk of dying from prostate cancer in males is approximately 3%. [2] Prostate cancer forms one of the top ten cancers in the studies of Thiruvanthapuram, Kolkota, Dehradun, and Eastern Rajasthan. [1],[3],[8] Regarding penile cancer, early circumcision decreases the risk, whereas, smegma, phymosis, and trauma increases the risk. [7],[8] Among the cancers of female reproductive organs, following cervix and breast, ovaries take seventh position (n = 46) in this study. It forms one of the top ten cancers in many studies. [1] We had only a few cases of endometrial and other female genital organ cancers. In our study liver cancers are more common in males (n = 30) than in females (n = 18). It can be attributed to the increased use of alcohol, smoking, and Hepatitis B virus (HBV) infection in this area. Laryngeal cancer was common in males (n = 25) in this study, which again can be attributed to smoking and alcohol. It is a common cancer in most of the studies in India. [1] Bladder cancer ranks tenth in our study and is common in males (n = 24). The various etiological factors reported are smoking, phenecetin, chemotherapy, naphythalamine-2, and S. hematobium. [2] It is more common in developed countries. [2] Rectal cancer takes ninth place among females (n = 22) in the present study. It is one among the top ten cancers in some South Karnataka districts, Salem, Thiruvanthapuram, and Eastern Rajasthan, where females predominate, whereas, in Srinagar and Ludhiana males predominate. [1],[6],[7],[8] It is more common in developed countries where there is an increased intake of fat, refined carbohydrates, and animal proteins, with low physical activity and low intake of fruits and vegetables. [2] Vitamin D, Calcium, Hormone replacement therapy (HRT) in Females, and non-steroidal antiinflammatory drugs (NSAID) / aspirin is protective against colorectal cancer. [2] Fecal occult blood test can be done as a screening test. [2] Melanoma takes tenth rank among female cancers (n = 20) in this study. It is usually due to increased exposure to the sun and commonly seen in manual labourers, in areas of extreme temperature. [2] Conclusion In the present study, oral cavity cancers were the commonest in both genders, followed by upper gastrointestinal cancers, which could be attributed to increased use of alcohol and tobacco. Rice is the staple food in this region, which can be associated with increased incidence of stomach cancer, as seen in other studies. However, the role of rice / carbohydrate-rich diet has to be proved by further epidemiological studies. In females, carcinoma of cervix predominated over breast cancer, as seen in developing countries. Thyroid cancers were more common in this region especially in females. Ours is a hospital-based study, which gives baseline data regarding the cancer profile, its association with probable risk factors that caus cancer, which help to plan cancer preventive / screening programs in future. However, awareness about the cancer pattern,prevention of risk factors, and improving the quality of life helps to decrease the incidence of cancer. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10041t4.jpg] [cn10041t5.jpg] [cn10041t1.jpg] [cn10041t2.jpg] [cn10041t3.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}