 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
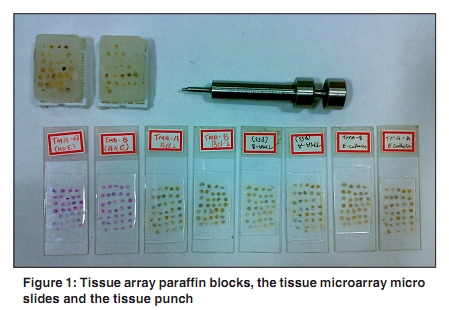
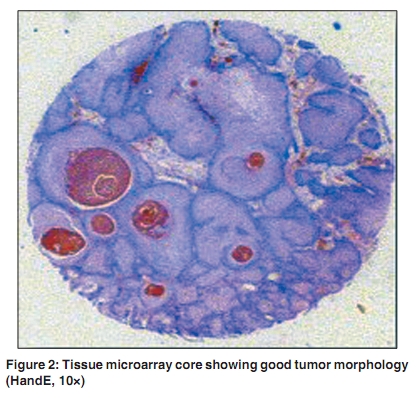
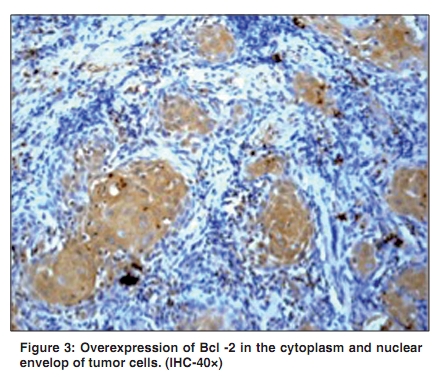
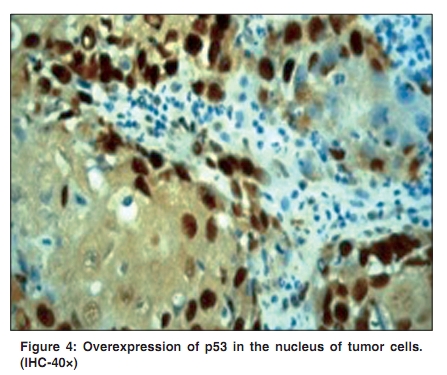
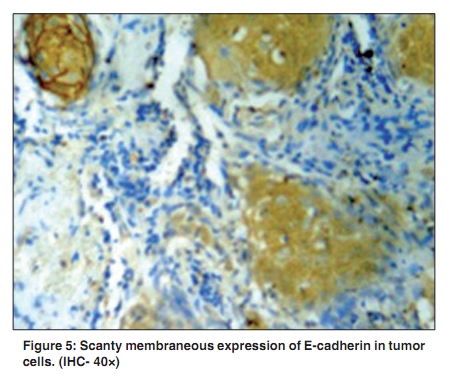
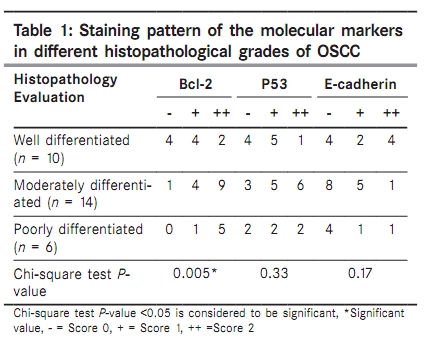
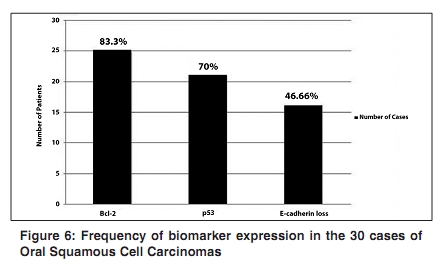
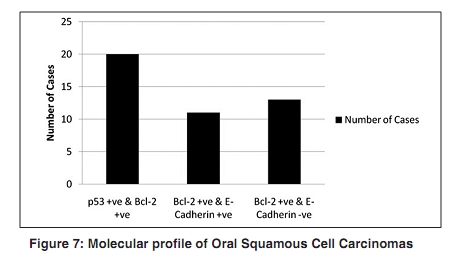
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 166-172 Original Article Molecular analysis of oral squamous cell carcinoma: A tissue microarray study Solomon MC, Carnelio S, Gudattu V1 Department of Oral Pathology, Manipal College of Dental Science, Manipal University, 1 Department of Biostatistics, Kasturba Medical College and Hospital, Manipal, Karnataka - 576 104, India Correspondence Address: Dr. Monica Charlotte Solomon, Department of Oral Pathology, Manipal College of Dental Science, Manipal University, Manipal, Karnataka - 576 104, India monicasolomon@yahoo.com Code Number: cn10042 PMID: 20448381 DOI: 10.4103/0019-509X.63013 Abstract Background : An intriguing aspect of Oral Squamous Cell Carcinomas (OSCC) is its behavioral disparity. Among patients who present with the similar clinicopathological features, some have a better prognosis than others. Identification of molecular alterations responsible for this may contribute to a greater understanding of tumor behavior. Tissue microarray (TMA) approach is a high throughput technology that enables analysis of multiple molecular targets simultaneously without causing any morphological alteration to tissue specimens. Keywords: Molecular screening, tissue microarray, oral squamous cell carcinoma Introduction Oral cancer is the sixth most common neoplasm in the World. [1] In India, oral cancer is the leading cancer among men and within the first five cancers of women, with an incidence rate of 12% of all cancers in men and 8% of all cancers among women. [2],[3] On the basis of a cancer registry, it is estimated that annually 75 000-80 000 new cases are reported in India. [4] The high incidence of oral cancer and pre-cancerous lesions in India has long been linked to the chronic use of tobacco in interesting forms like reverse smoking and incorporating tobacco in betel quid, besides smoking tobacco. [5] Despite advances in treatment, the 5-year survival has remained the same in the last 50 years. [6] Over the last two decades there have been important advances in the field of molecular biology. Numerous molecular markers have been identified and their roles in the development and progression of oral carcinomas have been established. Bcl-2 is a 25 kDa apoptosis regulatory protein that is located on the inner mitochondrial membrane, endoplasmic reticulum and the nuclear envelope. [7] Its expression has been associated with cellular proliferation, tissue development and morphogenesis. In addition, aberrant patterns of Bcl-2 expression are seen in various carcinomas. [8],[9] p53 is a 53 kDa nuclear phosphoprotein, which causes cell cycle arrest at G1-S cell cycle check point following damage to DNA. Overexpression of defective p53 protein is found to be an important event in the development of carcinomas including Oral Squamous Cell Carcinoma (OSCC). [10],[11] E-cadherin is a 120 kDa transmembrane glycoprotein that functions as cellular adhesion molecule in the presence of calcium. [12] Loss or reduction of the expression of this molecule has been found to be associated with invasion and metastatic behavior of oral cancers. [13],[14] Oral Squamous Cell Carcinoma (OSCC) like most other neoplasm consists of a heterogeneous cell population of varied biological behavior. Clinical and pathological parameters alone are not sufficient to determine the biological characteristics of the tumor. Besides that, it is clear that the expression of a single oncoprotein may not be a reliable biological indicator to predict patient outcome. Therefore, throughput analysis of multiple molecular markers is essential for a more accurate assessment of tumor behavior. The novel TMA technology enables multiple molecular targets to be evaluated rapidly and efficiently. In 1998, Kunonen and his collaborators [15] gave a new dimension to the conventional ′sausage′ method originally described by Battifora [16] for multiple tissue analysis. The application of this robust technique has emerged as a phenomenal breakthrough in cancer research. It is essentially a simple mechanical method wherein minute cylindrical tissue cores are taken from formalin-fixed paraffin-embedded (FFPE) ′donor′ tumor blocks and are subsequently arrayed on a ′recipient′ - TMA block. The principles of TMA, technical aspects of its construction and the application of this robust technology in head and neck cancer research have been described earlier. [17] Tissue microarray technology has been applied in several studies to demonstrate cellular alteration in OSCC. [18],[19],[20] Sadly, the application of this robust technology in cancer research in India has not yet been documented. Hence, the primary goal of this study was to construct a TMA using a simple custom-made design. Next, we examined OSCC with reference to its cell cycle regulation and cell-cell adhesion properties by analysing the expression of Bcl-2, p53 and E-cadherin using a systematic approach of IHC and TMA. Finally, we assessed the behavior of individual cases based on the expression of these molecular markers. Materials and Method Formalin-fixed paraffin-embedded (FFPE) tumor blocks of 30 histologically proven cases of OSCC were obtained from the departmental archives. Paraffin blocks of normal oral mucosa and that of breast carcinoma were also included as control specimens for the study. The clinicopathological details of all the patients were recovered from the departmental files. All cases that were selected were primary squamous cell carcinomas and had not undergone radiotherapy or chemotherapy prior to surgical excision. Fresh sections were obtained from all the FFPE blocks and stained with hematoxylin and eosin (H and E). The tumor sections were reviewed and areas with least tumor differentiation were identified and circled. Using the marked slide as a template, the morphological representative area on the matched tissue specimen was identified. Meanwhile, on the recipient paraffin block, punch holes of 2 mm diameter and at a distance of 1.5 mm from each other was made using a small metal needle. Next, two donor cores of 2 mm diameter each were obtained from the representative areas on the tumor block using a custom-made Handy tissue microarrayer (applied for patency protection). The tissue cores were removed from the punch with a Stylet. Finally, the donor cores that were obtained from the tumor samples were carefully inserted into the holes on the recipient block. In the same manner, two donor cores were also obtained from the control tissue blocks and arrayed on the recipient TMA block. As the cores were arrayed on the TMA block, their location on the array was recorded on custom-made Excel worksheets. The cores were arranged in a grid-like fashion in the recipient block. Thereby, two TMA blocks of 35 mm Χ 22 mm with an array of 34 tissue cores each, was constructed, which was eventually used for all further assays [Figure - 1]. The prepared TMA blocks were placed face down on a clean microscopic slide and warmed in an oven at 37ΊC for 15 min. This ensured that tissue cores adhered well to the walls of the holes in the array block. Following this, the array blocks were placed on a block of ice and cooled. A standard rotary microtome was set up and 5 ΅m thick sections were cut from the TMA blocks. The sections were stained with HandE to ascertain the morphology and tumor representation in the tissue cores [Figure - 2]. For immunohistochemistry, several 4΅m thick sections were cut from the TMA blocks and mounted onto APES, [3′aminopropylethoxysilane, (Sigma, Aldrich Chemical Co., St. Louis, MO, USA)] coated microslides. Endogenous peroxidase was blocked by treating sections with freshly prepared 3% H 2 O 2 in methanol for 20 min. For unmasking the epitomes the microslides were immersed in preheated 0.01 mM sodium citrate buffer (pH 6) and boiled in a pressure pot for 8 min. Slides were allowed to cool down in the citrate buffer until the pressure came down completely. Nonspecific antigens were blocked with 10% goat serum at room temperature for 30 min. The tissue sections were incubated with primary antibody Bcl-2 (clone 124, Dako, Cytomation, Denmark), p53 (clone D07, Dako, Glostrup, Denmark) and E-cadherin (clone NCH-38 Dako, Cytomation, Denmark) for 60 min in a humid chamber. The immune reaction was detected using streptavidin peroxidase system (Sigma, Aldrich Chemical Co, St Louis, MO, USA) and the reaction was developed with 3 3′diaminobenzidine tetrahydrochloride (Dako cytomation Denmark). Finally the sections were counterstained with Mayer′s hematoxylin and mounted with DPX. For the negative control, the tissue array sections were treated with normal goat serum instead of the primary monoclonal antibody. Analysis of immunohistochemical staining The analysis and scoring of the TMA microslides were carried out with a light microscope (Leitz Laborlux) at a magnification of 40Χ. The expression of the antigens investigated was evaluated in a semiquantitative manner. The expression of the markers in tumor cells in both the cores of each case was collectively scored. For Bcl-2, the cytoplasmic expression was considered and for p53 the nuclear expression was considered and was scored based on the following criteria: Score 0 (-) - < 10% of cells were positive Score 1 (+) - 10-50% of cells were positive core 2 (++) - >50% of cells were positive For E-cadherin, the immunohistochemical expression was scored as follows: Score 0 (-) - < 10% of cells showed membranous staining Score 1 (+) - 10 to 50% cells were immunoreactive Score 2 (++) - more than 50% of cells were stained positive Statistical Analysis Statistical analysis was carried out using the SPSS package (version 15). Mean (SD), minimum and maximum was used to summarize the age. Frequency with percentage was used to summarize the categorical variables. Chi-square test was used to find the association between the staining pattern of the makers (Bcl-2, p53 and E-cadherin) and the histopathological tumor grade. A P-value of less than 0.05 was considered to be statistically significant. Result This study was carried out to evaluate the expression of Bcl-2, p53 and E-cadherin in 30 histological proven cases of OSCCs. The age of patients ranged from 40 to 75 years. The mean age 57.8 and standard deviation being 9.5. Of the 30 cases, 19 were male patients and 11 were female patients. Based on the pathology, 10 of the cases were Well-differentiated Squamous Cell Carcinomas (WDSCC), 14 cases were Moderately Differentiated Squamous Cell Carcinomas (MDSCC) and 6 cases were Poorly Differentiated Squamous Cell Carcinomas (PDSCC). Cytoplasmic expression of Bcl-2 [Figure - 3] was evident in 25/30 (83.3%) cases. Among the 10 cases of WDSCC, 6 (60%) cases were positive for the expression. Of the 14 cases of MDSCC, 13 (92%) cases were positive for the expression. All the 6 (100%) cases of PDSCC were positive for the expression. The differences between the percentage of cases that expressed Bcl-2 among the different grades was found to be statistically significant (P = 0.005). Nuclear expression of p53 expression [Figure - 4] was evident in 21/30 (70%) cases. Among the 10 cases of WDSCC, 6 (60%) cases were positive for the expression. Among the 14 cases of MDSCC, 11 (78.6%) cases were positive for the expression. Among the 6 cases of PDSCC, 4 (66.6%) cases were positive for the expression. There was no significant difference between the percentages of the cases that expressed the biomarker between the different grades of the tumor (P = 0.33). Membranous expression of E-cadherin [Figure - 5] was seen in 14/30 (46.6%) cases. Among the 10 WDSCC, 6 (60%) cases were positive for the expression. Among the 14 cases of MDSCC, 6 (42.8%) cases were positive for the expression. Among the 6 cases of PDSCC, 2 (33.4%) cases showed a positive expression. There was no significant difference between the percentages of the cases that expressed the biomarker between the different grades of the tumor (P = 0.17). In this study among the three biomarkers that were evaluated, Bcl-2 was the most frequently expressed biomarker. In addition, the frequency of Bcl-2 expression increased with decreasing degree of cell differentiation. The staining pattern of the molecular markers in the different grades of OSCC along with the Chi-square test P value for association of the marker expression with tumor grade is given in [Table - 1]. The frequency of the biomarker expression among the 30 cases of OSCC is given in [Figure - 6]. Molecular profile of all the OSCC cases is given in [Figure - 7]. The association of the tumor behavior with respect to the molecular profile is given in [Table - 2]. Discussion Tissue microarray technology has been touted as one of the most noteworthy developments in histopathological techniques in recent times. The combination of TMA with IHC is a powerful approach to detect molecular alteration involved in the pathway of carcinogenesis. Tissue Microarrays have immense potential to investigate a large number of different protein molecules in a shorter time frame. Currently, there are several tissue microarrayers that are either manual or automatic and commercially available. The most popular being the Beechers Tissue arrayer (San Prairie, Wisconsin, USA). These precision instruments carry punch units of core diameter in the range of 0.6, 1 and 2 mm. Most researchers have favored the 0.6 mm diameter, as it is easy to use and at that diameter several hundred cores can be inserted into a single TMA blocks. [15],[21],[22] However, a tumor tissue with a core diameter of 2 mm cylinder size affords recognizable histological features and the tissue area available for evaluation is enlarged by a factor of 10 as compared to the smaller diameter tissue cores. [23],[24] With this thought, we fabricated this tissue punch with a core diameter of 2 mm. In addition, this tissue punch is a cheap alternative for practical use in any laboratory, where sophisticated facilities are not readily available. The validity of tumor cores to reliably represent protein expression as in full tissue sections have been evaluated in head and neck carcinomas. [25],[26] In order to verify this in Indian OSCC, we compared the protein expression in tissue cores with those in whole tissue sections. We found satisfactory concordance in the protein expression in tissue cores and the whole sections. Deregulations in the apoptotic pathways have been linked to the biology and pathogenesis of OSCCs. In this study, Bcl-2 was the most frequently expressed biomarker, and was expressed in 83.3% of cases. A significant inverse relationship was found between the expression of Bcl-2 and degree of differentiation of the carcinoma (P = 0.005) [Table - 1]. Previous studies have also reported this inverse relation of the expression of Bcl-2 with the degree of differentiation in OSCC. [27],[28] Bcl-2 protein is known to be topographically restricted to cells in proliferative zones and cells with longer life spans. [29] As the degree of differentiation decreases, number of cells in the tumor that express Bcl-2 is greater. These tumor cells evade apoptosis and achieve unrestrained cell survival. Nuclear accumulation of p53 protein in tumor cells indicates an alteration in the cell cycle regulation and confers a proliferative advantage to the neoplasm. [30] In this study, nuclear expression of p53 was observed in 21/30 (71%) cases. Additionally, we found that 20/30 (66.6%) cases were positive for both p53 and Bcl-2. The alteration (loss of function) of p53 possibly causes the aberrant Bcl-2 expression. The overexpression of Bcl-2 and the loss of function of p53 (which is also represented by its expression) play an important role in the tumorigenesis of oral cancers by resulting in defective apoptosis and subsequent tumor progression of the tumor. [31] In an earlier study by Teni et al. on Indian Squamous Cell Carcinomas, 30% of the cases also demonstrated both p53 and Bcl-2 expression. [32] Although Chiang et al.[33] had found that p53 negative tumors had a better prognosis than p53 positive tumors, we found that, of the tumors that expressed both these biomarkers (Bcl-2 and p53), 14/20 (70%) cases demonstrated a favorable response to treatment. Further, in our study, we found that 13/30 (43.3%) cases were positive for Bcl-2, but demonstrated a loss of E-cadherin expression. A four-year follow-up of these cases showed that recurrence/metastasis developed in 8/13 (61.5%) cases [Table - 2]. Although Bcl-2 expression may not always be directly linked to tumor differentiation, tumors with active proliferative potential can express this proto-oncogene. [34] While, reduced staining for E-cadherin is found to correlate with the invasive and metastatic behavior of SCCs. [35] Thus, in these cases the high proliferative potential and the susceptibility to develop metastasis due to the loss of E-cadherin could have accounted for the poor prognosis. Bankfalvi et al. have also shown that there was a significant association of E-cadherin loss and poor survival of oral cancer patients. [36] Interestingly, expression of Bcl-2 has been found to decrease the level of functional E-cadherin, thereby interfering with junction formation. [37] Our four-year follow-up data has also shown that 7/11 (63.6%) of the patients with tumors that were positive for Bcl-2 and E-cadherin expression have been disease free following treatment. Although, common pathways are said to regulate the intercellular adhesion and cell proliferation, the functional interaction between homo-dimers and hetero-dimers of the Bcl-2 family modulates the intrinsic activity of the molecules that belong to this family. [38] Hence, in these tumors although Bcl-2 was expressed, E-cadherin was also present and expressed at the cell junctions. Thus, in these tumors, though there were Bcl-2 expressing neoplastic cells, due to the presence of E-cadherin, the epithelial cells were bound to each other and their integrity was maintained. Literature data has also shown that patients with increased levels of E-cadherin appeared to have a favorable survival rate. [12] However, in our study we also observed that 5/13 patients with tumors that expressed Bcl-2 but with loss of E-cadherin expression presented with a good prognosis. In these cases other molecules associated with cell junction formation such as catenins, desmogleins, desmoplakins and others might have contributed to this behavior. Alternatively, there were 4/11 patients with tumors that expressed both Bcl-2 and E-cadherin but they developed recurrence and metastasis. The pathogenesis of oral squamous cell carcinomas involves a myriad of molecular pathways, and hence, the molecular alteration underlying this character among tumors is obscure and needs to be further investigated in a larger series of cases. This preliminary study was an attempt to apply the novel tissue microarray technology in cancer research. However, studies are underway on a larger sample size to confirm the findings of this study. Further studies are also being designed to arrive at ′molecular profiles′ of tumors, which will enable categorization of patients into more realistic risk groups. Tissue microarray technology has the potential to accelerate molecular studies that seek to associate molecular changes and clinicopathological characters of tumors. This novel technology also paves the way to carry out wide studies on cancerous lesions that will lead us to a precise knowledge of the molecular alteration involved in the biology of the tumor. Tissue microarrays can be easily constructed using simple cheap custom-made devices such as this tissue punch. We, encourage research groups of small-sized laboratories to employ tissue microarray technology as a routine cancer research tool. Acknowledgments The authors acknowledge the financial support offered by the International Union against Cancer. Dr Monica Charlotte Solomon was awarded a UICC ICRETT fellowship (ICR/05/23) for the project ′Immunohistochemical analysis of tumor markers during the development and progression of head and neck cancers using tissue microarray: A systematic approach,′ which was carried out at the Department of Pathology, University of Chicago, IL 60637-1470, USA, under supervision of: Dr Mark W Lingen; Mr Alwin Niranjan Bangera, Department of Mechanical Engineering, Manipal Institute of Technology, Manipal, Karnataka, 576104, India for fabricating the tissue punch; Leslie E Martin, Senior Research Technologist, Technical director CRC core laboratory;Biospecimen Bank, Department of Pathology, University of Chicago, IL 60637-1470 USA; Dr Raghu AR, Professor, Department of Oral Pathology, Manipal College of Dental Sciences, Manipal, Karnataka, India; Dr Muruganandan J, Post Graduate Student, Department of Oral Pathology, Manipal College of Dental Sciences, Manipal, Karnataka 576104, India References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10042t1.jpg] [cn10042f3.jpg] [cn10042f6.jpg] [cn10042t2.jpg] [cn10042f5.jpg] [cn10042f4.jpg] [cn10042f7.jpg] [cn10042f1.jpg] [cn10042f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}