 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
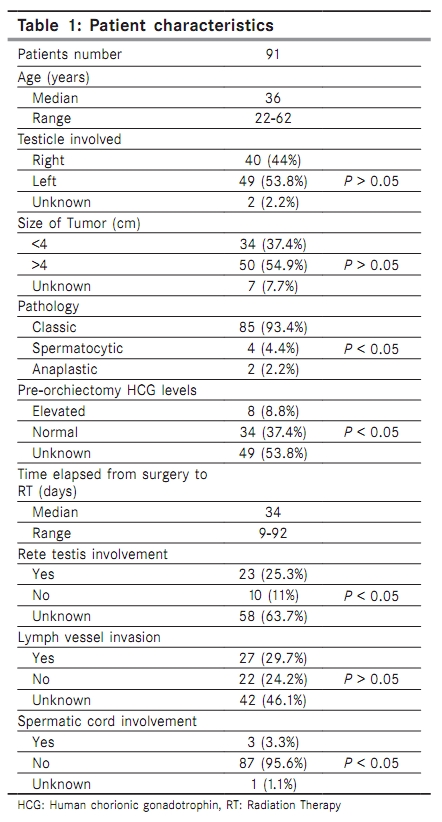
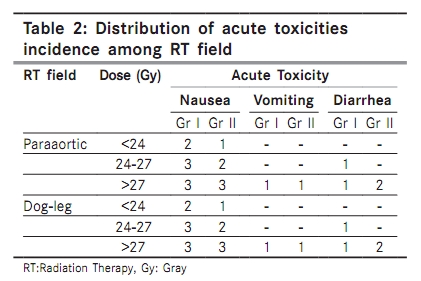
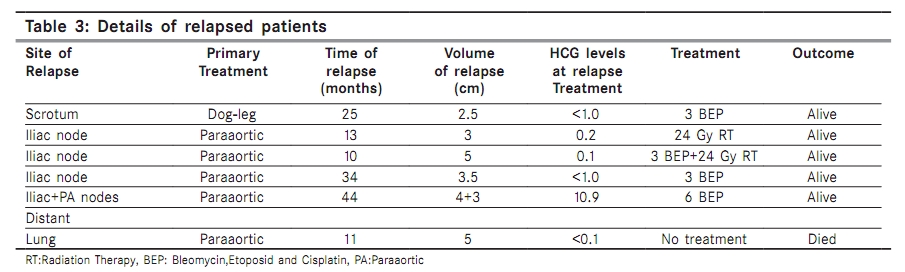
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 179-183 Original Article Radiotherapy for stage I seminoma of the testis Yoney A, Yildirim C, Isikli L, Akboru H, Unsal M Department of Radiation Oncology, Okmeydani Training and Research Hospital, Istanbul, Turkey Correspondence Address: Dr. Adnan Yoney, Department of Radiation Oncology, Okmeydani Training and Research Hospital, Istanbul, Turkey adnan@yoney.net Code Number: cn10044 PMID: 20448383 DOI: 10.4103/0019-509X.63017 Abstract Background : After orchiectomy in stage I seminoma the standard is adjuvant radiation therapy. We analyzed the patients retrospectively to evaluate the contributions of the treatment volume and dosage to treatment outcomes.Materials and Methods : Between January 1999 and December 2005, 91 stage I seminoma patients with a median age 36 (range;22-62) applied to our center, who were treated using anterior-posterior parallel opposed fields with linear accelerator or Co60 after orchiectomy. Twenty-five (27.5%) patients received irradiation to the paraaortic and ipsilateral pelvic nodes, and 66 (62.5%) patients only received to paraaortic nodes. Results : With a follow up time of median 57 months (range; 27-104), paraaortic nodes treated group had 4 relapses (6%) - 3 of them pelvic, one of them both pelvic and paraaortic. Both paraaortic and ipsilateral nodes irradiated patients had only one relapse (4%) (P = 0.726). While the 5 year overall survival (OS) is 98.8%, it is 100% in the dog-leg group and 98.4% in the paraaortic group (P = 0.548). Univariate analyses of OS and Disease Free Survival (DFS) showed that there is no statistically significant difference related to factors as age, histologic subgroup, tumor size, rete testis involvement, radiotherapy (RT) fields, dose ranges and the therapy device. Conclusion : Adjuvant RT approach is the preferred for non-compliant low risk patients as well as intermediate and high risk patient in stage I seminoma. 20 Gy/ 10 fractions/ 2 weeks RT is the adequate treatment. Keywords: Stage I seminoma, risk-adapted therapy, radiotherapy, paraaortic field, dog-leg field Introduction Pure seminomas composes 60% of the testiculer tumors which are most commonly seen in males between ages 20 to 35 and 70-80% these cases are stage I tumors. [1],[2] Management options of stage I seminoma include radiotherapy (RT), surveilance (SU) or chemotherapy (CT) after orchiectomy. For the past 65 years, patients with stage I seminoma have been treated with adjuvant RT. [3] While we achieve 95-100% local control and survival rates this also brings along higher risks of early and late gonadal toxicities, secondary malignancy as well as highered risk of cardiovascular diseases. [4],[5] As application of para-aortic field only (without pelvic field) [6],[7] or delivering decreased RT doses at only about 20 Gy [8],[9] aim to decrease specially the early toxicity; other modalities besides RT are in search to control the developing late risks. SU [10],[11] or single-agent carboplatin [12] are preferred for this reason. In our study the effects of RT field and dose modifications as well as the effects of known prognostic factors on local control and survival are taken as the primary end points, while the rates of toxicity following RT formed the secondary end point and results are retrospectively analised in stage I seminoma patients who are treated with RT in our center between years 1999-2005. Materials and Methods The present study was performed retrospectively in 91 stage I patients with histologically proven pure seminoma. All patients received radical inguinal orchiectomy and treated with RT. Routine staging consisted of clinical examination, chest radiography, computed tomography (CT) scan of the chest, abdomen and pelvic and measurement of lactate dehydrogenase (LDH), alpha-fetoprotein (AFP) and beta-human chorionic gonadotropin (BHCG). Increased preoperative levels of BHCG were acceptable, but either the persistance of increased postoperative BHCG level or any pre-or postoperative elevation of AFP were considered exclusion criteria. After surgery irradiation started within a median of 34 days (range; 9-92). The radiation fields extended from the Thoracal 10 vertebral level to the Lomber 5 vertebral level in using para-aortic field. Using dog-leg field, the radiation field extented from the Thoracal 10 vertebral level to the obturator foramen, including the ipsilateral iliac and pelvic lymph nodes. Para-aortic and ipsilateral pelvic nodes irradiated in 25 (27.5%) patients, 66 (62.5%) got only para-aortic irradiation. RT dose was median 26 Gy (range;19.6-36). Radiation given using anterior-posterior opposed fields with 6-18 MV linear accelerator or Co60 devices. At the dog-leg type a median of 25.6 Gy (range; 19.6-36) RT doses were used and in para-aortic type it was 26 Gy (range; 19.6-30.6). In all cases daily 1.8 Gy fractionations were used. Complications related with the skin, bowel and bladder were classified according to Radiation Therapy Oncology Group (RTOG). Patients were scheculed for a follow-up appointment after RT was completed. Follow-up was performed quarterly for the first two years, bi-annually for the next theree years and annually threafter. Evaluation of patients included clinical examination, routine blood biochemistry, chest radiography and CT scans of the thorax, abdomen and pelvis and tumor markers. The patients who did not attend the control periods were called up by phone or written letters and information concerning their last situations where updated. Survival statistics were made over 87 patients except the 4 inaccessible cases. OS time is calculated as the time after the radiotherapy to last control; DFS time calculated as the time after radiotherapy to local recurrence date. Median follow-up was 57 months (range; 27-104).The contact was lost with 4 (4.4%) patients during follow-up after treatment. SPSS (Statistical Package for Social Sciences) for Windows 10.0 program was used for statistical analysis to evaluate the results obtained. In addition to the defining statistical methods (median, standard deviation, frequency), one-way Anova test was used for comparing groups with parameters showing normal distribution in quantitative data and Tukey HDS test was used to determine the group that accounts for the difference. For qualitative data, chi-square test and Fisher′s exact chi-square test were used. Kaplan Meier survival analysis was used for survival analyses and Log Rang test was used for comparing survival data. A P-value < 0.05 was considered significant. Results General characteristics of patients are shown in [Table - 1]. Median age is 36 (range; 22-62). Two patients had tumors in the contra lateral testis before. One of them had already a seminoma 22 years before and the other had already a non seminomatous tumor 9 years ago. There is no difference with right and left sides in terms of localization. Classic type of seminoma was seen in 94 percent of cases. Before surgery, HCG levels were examinated in 46% and elevation of HCG was observed in 9% of patients. For the Radiation Therapy Oncology Group (RTOG) toxicity criteria grade 1 gastrointestinal (GI) toxicity was seen in 31 patients (34%), grade 2 GI toxicity was seen in 9 patients (9%). 51 patients had no acute toxicity. Most frequent GI toxicities were nausea and vomiting present in 28 patients (30%). Diarrhea occurred in 7 (7%) patients. Paraaortic and dog-leg fields had no differences in terms of acute toxicity (P = 0.686). However the toxicity rate is proportionally increased with the dose applied [Table - 2]. These symptoms were tolerable and managed with simple medications. No late toxicity was seen and no second malignancy developed in the follow-up period. In follow up period with a median 57 months (range; 27-104), 90 out of 91 patients are still alive without any recurrences. Five patients had recurrence after treatment. Local control rate is 94.5%. One of the relapses occurred in the dog-leg field (4%), four of them occurred in the paraaortic field (6%). There is no statistically significant relation between treatment fields and recurrences (P = 0.726). Three of the recurrences occurred in the ipsilateral pelvic nodes and the other occurred both at paraaortic and pelvic nodes [Table - 3]. There is no pelvic surgery history determined in the relapsed cases. After local recurrence 3 of the patients received chemotherapy alone, one of them received 24 Gy radiotherapy alone and the other received both chemotherapy and 25 Gy radiotherapy and currently all of them are alive and have no disease. Distant metastases developed only in one patient (1%) in the lung in the 11 month. This patient refused the chemotherapy after the metastases and died in the 4. month of metastases. HCG elevation was detected only in one of the 6 patients (16.6%) with locally and distant relapsed disease. Five year OS is 98.8% (mean: 102.98 ± 1.02). In the dog-leg field group OS is 100% and in the paraaortic field irradiated group this rate is 98.4% (P = 0.548). DFS at 2 and 5 years is 96.5% and 89.7% respectively (mean: 96.31 ± 2.60). In univariate analysis when; the OS and DFS are searched no statistically significant difference has been seen in terms of age, histologic subgroup, tumor size, radiotherapy field, the time between operation and radiation, radiotherapy duration, dose ranges and treatment devices. When the existence of disease analyzed by age, 5 year OS is 94.1% in patients older than 50 years and is 100% in patients younger than 50 years (P = 0.1021). In the classic type seminoma, 5 year OS is 98.8% while it is 100% in the other two subtypes. When analyzed by tumor size, OS is 100% in those greater than 4 cm and 98.2% in those smaller than 4 cm (P = 0.2752). In presence of the rete testis invasion OS is 100%, while it is 98.8% in its absence (P = 0.8492). In cases with time between orchiectomy and radiotherapy shorter than 30 days OS is 100%, and is 94.1% in cases with time longer than 30 days (P = 0.5676). OS is 100% in the dog-leg group and 98.4% in the paraaortic group (P = 0.5369). If the duration of radiotherapy is 20-30 days OS is 97.8% and 100% when longer than 30 days. OS is equally 100% in groups with doses, lower than 24 Gy and higher than 27 Gy while 97.6% in 24-27 Gy interval group (P = 0.5369). When the linear accelerator used OS is 96.7%, and 100% if the Co60 device is used (P = 0.1681). Discussion Excellent local control and survival rates are achieved with RT after orchiectomy while higher risks of early and late gonadal toxicities, secondary malignancy as well as highered risk of cardiovascular diseases still stands as a problem. Recent approaches of choice are reducing the radiotherapy fields or doses, SU and CT. [13],[14] Historically all the lymphatic pathways were irradiated. In recent years only the paraaortic area irradiated as being the first lymphatic drainage of testis and have the same local control and survival rates with dog-leg RT. [15] If there is no pelvic surgery history paraaortic stripe field irradiation is adequate. Should there is a pelvic surgery history which causes a lymphatic pathway damage or change of course, RT has to be delivered with dog-leg fields. In our study there is no statistically significant difference between these two groups in terms of local control (P = 0.726) and survival (P = 0.548). Reducing the dose of RT is another choice to avoid morbidity which can occur within a long follow-up period. Reducing doses to 20-24 Gy, there is no difference in local control and survival. In our study similar findings are achieved with doses over 20 Gy. Although spermatositic type seminoma is cited to have better outcomes in literature, we had no statistically significant difference in terms of different histological subtypes. Additionally, univariate analyses of the other known prognostic factors such as, tumor size greater than 4 cm; rete testis invasion; lymph vessels involvement; spermatic cord invasion; LDH elevation yield no effects on local control and survival. The time between surgery and radiotherapy; radiotherapy duration and RT device type have also no effects on local control and survival. Paraaortic and dog-leg fields had no differences in terms of acute toxicity (P = 0.686). Reducing the RT field doesn′t effect on the acute toxicity however increasing the dose proportionally Increases the acute toxicity. No late toxicity was seen and no second malignancy and no cardiovascular diseases developed in the follow-up. An increased risk of second non-testicular cancers after RT has been documented in various studies and since this increased risk is expressed in series with a follow-up time of 10 to 15 years, the long term survivors of seminoma treated with RT are also at significant excess risk of death as a result of cardiac disease although they are not apparent in our study which has relatively a shorter follow-up period with a median of 57 months (range;27-104). [16],[17] This is the deficiency of our study. If the follow-up period would have been longer, we would probably see the contribution of these parameters better. SU has become increasingly recommended as the association between RT and second malignancies has emerged. But the local recurrence rates are 16-20% in this approach. Using RT reduces the recurrence rates 5-6 folds down to 3-4%. [18] Warde et al. [19] found tumor size> 4 cm and rete testis involvement to predict the rate of relapse (risk 12% for patients without feature, 16% with one feature present and 32% with both features present). Furthermore, this approach is not recommended when the tumor size is greater than 4 cm and/or rete testis invasion exists. In our clinic follow-up with no RT is not recommended because of the higher relapse rates and our patients had larger tumor sizes greater than 4 cm. Other main concern with SU is patient compliance with follow-up. 21% of seminoma patients on SU were lost to follow-up after a median of 5.5 years. [20] At least 5% of relapses occur after 5 years, suggesting that non-compliant patients will present with more advanced disease and need more intensive treatment. [21] Adjuvant CT using Carboplatin has been investigated as an alternative strategy to RT in stage I seminoma. With mature follow-up, one or two courses of Carboplatin is safe, less acutely toxic and as effective as RT. [22] But long term results will show if it can replace RT or not. [23],[24] To deal with the choice of existing alternatives a such called "risk-adapted approach" is suggested to determine the treatment management. [25] A risk-adapted approach to treatment management has been reported by the Spanish Germ Cell Cancer Cooperative Study Group with SU reserved for low risk patients and adjuvant therapy for intermediate and high risk patients. [26],[27] In conclusion; SU is the recommended treatment option in stage I seminoma patients who are compliant and at low risk. Adjuvant RT approach is the preferred approach for non-compliant or those unwilling to go on SU with low risk patients along with intermediate and high risk patients. 20 Gy/10 fractions/2 weeks paraaortic RT is the adequate treatment. Should there is a pelvic surgery history the dog-leg field is the field of choice. Adjuvant CT should be restricted to study settings until longer follow-up is available. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10044t1.jpg] [cn10044t2.jpg] [cn10044t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}