 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
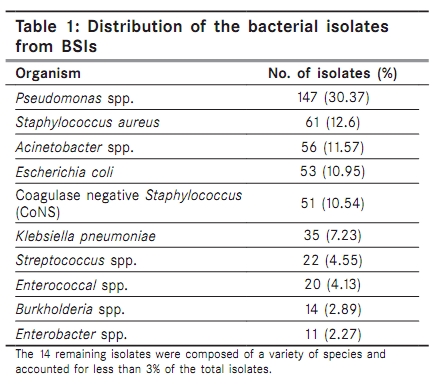
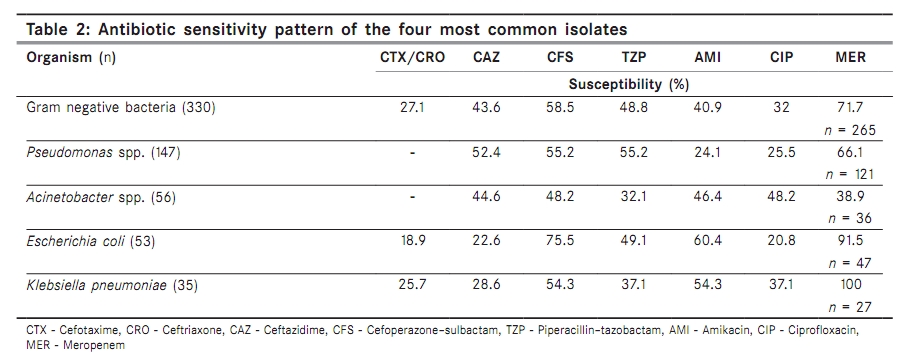
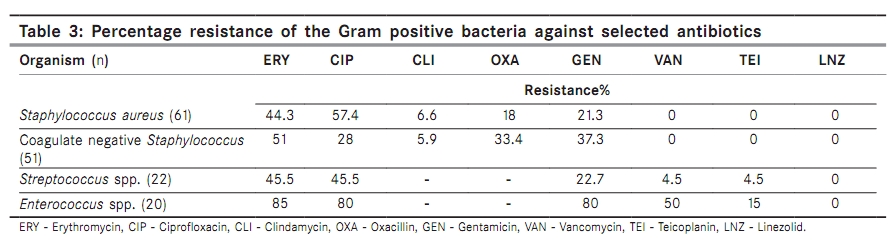
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 184-188 Original Article Blood stream infections in cancer patients: A single center experience of isolates and sensitivity pattern Prabhash K, Medhekar A, Ghadyalpatil N, Noronha V, Biswas S, Kurkure P, Nair R, Kelkar R Department of Medical Oncology, Tata Memorial Hospital, Mumbai, Maharashtra, India Correspondence Address: Dr. Kumar Prabhash, Department of Medical Oncology, Tata Memorial Hospital, Mumbai, Maharashtra, India kp_prabhash@rediffmail.com Code Number: cn10045 PMID: 20448384 DOI: 10.4103/0019-509X.63019 Abstract Background : Up to 10% of patients who develop a nosocomial blood stream infection (BSI) in the hospital have an underlying malignancy. The treatment of infections in patients with malignancy often relies on the use of established guidelines along with the consideration of the local microbiology and antibiotic sensitivity patterns of possible etiologic agents. Keywords: Antibiotic sensitivity, blood stream infections Introduction Patients with cancer are predisposed to infection and often the focus of infection is not evident. Up to 10% of patients, who develop a nosocomial blood stream infection (BSI) in the hospital have an underlying malignancy. [1] Blood stream infections increase the length of hospital stay, cause significant morbidity and mortality and increase the cost of care. The crude mortality rate for BSIs in cancer patients ranges from 18 to 42%. [2],[3],[4],[5] The treatment of these infections often relies on the use of empirical therapy based on established guidelines with due consideration to the local microbiology and antibiotic sensitivity patterns. This study attempts to identify the likely etiologic agents and the antibiotic sensitivity profile of BSIs in cancer patients at a single center. Material and Methods This was a retrospective study conducted at a tertiary care hospital for cancer patients. We analysed all samples (from neutropenic and non-neutropenic patients) sent for bacterial culture from the Medical Oncology services of the hospital during the year of 2007. Samples that represented blood stream infections were identified. These samples included peripheral blood, blood drawn through catheters and catheter tip cultures from patients with an appropriate clinical syndrome. The bacterial isolates from these samples were identified by routine biochemical reactions. The in vitro antibiotic sensitivity pattern of these isolates was determined by the Kirby Bauer′s disc diffusion method. Choice of antibiotic disks used was determined by Clinical and Laboratory Standards Institute (CLSI) guidelines. [6] Extended spectrum beta-lactamase (ESBL) production was confirmed by CLSI recommendations using cephalosporin-clavulanate combination disks. A difference of ≥5 mm between zone diameter of either of the cephalosporin disks and their respective cephalosporin-clavulanate disk was taken to be phenotypic confirmation of ESBL production. We used cefotaxime (30 μg), ceftazidime (30 μg) and ceftazidime/clavulanic acid (30 μg/10 μg) disks for ESBL determination. [6] An analysis of the microbiological spectrum and the antibiotic sensitivity pattern of the bacterial isolates were performed. Statistical Methods The isolates were mapped on the WHONET 5.4 software and analysed using the same program. Results A total of 990 isolates were cultured from all samples sent from in-patients admitted in the Medical Oncology services. Of these, a total of 516 isolates were obtained from the sample sites that represented blood stream infections. Isolates having identical antibiograms obtained from a single patient during the same hospitalization were considered once. As a result 484 isolates were analyzed. There were 154 Gram positive bacterial isolates (31.81%) and 330 Gram negative isolates (68.18%). Of these isolates, 336 were from peripheral blood (69.42%), 101 from blood drawn through a peripherally inserted central catheter (20.87%), 35 from catheter tip cultures (7.23%), 11 from blood drawn from a central catheter (2.27%) and 1 from blood drawn through a permanent catheter (0.2%). The contribution of the most prevalent bacterial isolates is given in [Table - 1]. The most common bacterial isolates were Pseudomonas spp. (30.37%), Staphylococcus aureus (12.6%), Acinetobacter spp. (11.57%) and Escherichia coli (10.95%). Staphylococcus isolates accounted for 72.73% of all Gram positive isolates, with 61 S. aureus isolates and 51 coagulase negative Staphylococcus spp. There were 21 (13.64%) isolates belonging to Streptococcus spp. and 20 (12.99%) to Enterococcus spp. The majority of the Gram negative bacteria were non-lactose fermenters (62.24%) with the Pseudomonas spp. and Acinetobacter spp. accounting for 147 and 56 isolates, respectively. Of the remaining Gram negative isolates, the contribution of E. coli isolates was 53 (16.06%) and that of Klebsiella pneumoniae was 35 (10.61%). Extended spectrum beta-lactamase production was tested in isolates from the Enterobacteriaceae group and was detected in 50 of them (15.15%). Among ESBL producers, 27 were E. coli (50.94% of E. coli isolates), 22 K. pneumoniae (62.86% of K. pneumoniae isolates) and one Enterobacter cloacae (9.09% of Enterobacter spp. isolates). Of all ESBL producers, 43 isolates were isolated from peripheral blood culture (86%) and 7 from blood drawn through a peripherally inserted central catheter (14%). The antibiotic sensitivity pattern of the most prevalent Gram negative bacteria is given in [Table - 2]. There was a high degree of resistance to the cephalosporins with only 27.1% of the Gram negative isolates being sensitive to the third generation cephalosporins, namely ceftriaxone and cefotaxime. The overall activity of the anti-pseudomonal cephalosporin, ceftazidime (CAZ), was better at 43.6%. However, this was due to its expectedly better anti-pseudomonal activity (52.4%). The susceptibility of E. coli and K. pneumoniae isolates of the third generation cephalosporins ranged between 18.9 to 22.6 and 25.7 to 28.6% v/s, respectively. The beta-lactam/beta-lactamase inhibitor combinations fared better in the overall activity against Gram negative bacteria [48.8% susceptibility for piperacillin-tazobactam (TZP) and 58.5% for cefoperazone-sulbactam (CFS)]. The sensitivity of Pseudomonas spp. to the combination antibiotics was comparable to that of ceftazidime (55.2% v/s 52.4%), however the activity of the beta-lactam/beta-lactamase inhibitors against E. coli isolates was much better (75.5% for CFS; 49.1% for TZP; 22.6% for CAZ). However, poor efficacy of beta-lactam combinations against the Acinetobacter spp. was found (32.1% for TZP and 48.2% for CFS). Meropenem was the most effective antibiotic and was active against 71.7% of the Gram negative bacterial isolates. There was no resistance documented against Klebsiella pneumoniae but resistance among E. coli was emerging (8.5%). It was the most active antimicrobial agent against Pseudomonas spp. (66.2%), however activity against Acinetobacter spp. was poor (38.9%). The aminoglycosides and quinolones showed variable activity. The overall activity against all Gram negative bacterial isolates tested was poor (32% susceptibility for ciprofloxacin and 40.4% for amikacin). There was a high degree of resistance among the Pseudomonas spp. for both antibiotics (74.5% resistance against ciprofloxacin and 75.9% for amikacin). The poor activity of ciprofloxacin against E. coli (20% susceptible) was disconcerting. The antibiotic sensitivity patterns for the Gram positive organisms revealed that linezolid was the most active agent. All the bacterial isolates tested were sensitive to linezolid and no resistance was documented. The activity of ciprofloxacin and erythromycin against the various Gram positive bacterial isolates was variable but in general suboptimal. Percentage of antibiotic resistance for Gram positive organisms is given in [Table - 3]. Oxacillin resistance was observed in 18% of S. aureus isolates and 33.4% of coagulase negative Staphylococcus isolates. All these isolates were sensitive to vancomycin and teicoplanin. Clindamycin resistance was low among Staphylococcus isolates and was documented among 6.6% of S. aureus and 5.9% of coagulase negative Staphylococcus isolates. Vancomycin resistant enterococci accounted for 50% of the Enterococcus spp. isolates. Teicoplanin resistance was evident in 15% of the Enterococcus isolates and an additional 35% Enterococcus isolates showed intermediate sensitivity. Discussion Blood stream infections are a cause of significant morbidity and mortality in cancer patients. The incidence of BSIs among neutropenic patients is 11-38%. [7],[8],[9] The causative organisms of BSIs have changed over time. In the 1960s to the 70s, Gram negative bacteria were more predominant causative agents but over the last few decades there has been a shift toward predominance by Gram positive bacteria. [1] There have been reports suggesting 70-81% of the bacteria isolated from BSIs are Gram positive. [10],[11] Our study however revealed that Gram negative bacteria were predominant. This has been an observation among similar studies done in patients in the developing countries. [12],[13],[14],[15],[16] The reasons for this could be the relatively lower use of indwelling catheters and other portal devices as well as low utilization of prophylactic antibiotic regimens in neutropenic patients. [17] Our institute does not use empirical antibiotics for prevention of bacterial infections among cancer patients, and the use of long duration indwelling catheters is generally restricted to patients with acute myeloid leukemia for the duration of high dose cytarabine therapy. The high occurrence of non-lactose fermenters especially Pseudomonas spp. and Acinetobacter spp. was of concern. Both of these bacteria are associated with a high degree of resistance to antibiotics. Blood stream infections with P. aeruginosa have been associated with increased mortality in some studies. [18],[19] Acinetobacter spp. have emerged as prominent multidrug-resistant bacteria in several intensive care units all over the world, and their occurrence in the setting of malignancy could be disastrous. There have been no studies, to our best knowledge, that have had such a high burden of BSIs due to non-lactose fermenters. It is probable that low utilization of home-based chemotherapy meant longer and more frequent hospitalization at our institute, and concomitant greater risk of acquisition of these hospital-based bacterial infections. The occurrence of methicillin-resistant S. aureus (MRSA) was low (18%) in our study; also there were fewer oxacillin-resistant (33.4%) coagulase negative Staphylococcus (CoNS) isolates. This is rather different from prevalence rates in most other studies. [12],[13],[14],[15],[16],[20] This suggests that the utilization of empirical vancomycin at our institute must be thoroughly scrutinized. The indiscriminate use of vancomycin has promoted resistance and this is evident by the high occurrence of vancomycin-resistant Enterococcus isolates (50% of all Enterococcus isolates in the study). Strict regulation of the use of vancomycin should therefore be considered in areas where there is a low prevalence of MRSA. The poor activity of the primary empirical agents for infections in cancer namely ceftazidime and piperacillin-tazobactam (43.6 and 48.4% susceptibility, respectively) is alarming. The high resistance to amikacin (59.1%) further compounds the problem. The only available alternative antimicrobial agents are carbapenems. But even here resistance has been documented high (28.8%). The poor activity of meropenem against Pseudomonas spp. and Acinetobacter spp. is especially distressing. This is a grim situation and there is an urgent need for the development of newer agents for the treatment of Gram negative infections. While polymyxin, chloramphenicol and cotrimoxazole are being revisited as possible choices for the treatment, there remains a growing requirement for novel agents. [21] Doripenem, tigecycline and ceftobiprole are now available but with the degree of resistance we have encountered in this study, it is a matter of time before these antibiotics are exhausted. Sound hospital infection control practices, decreased reliance on hospital-based care and restricted antibiotic use would go a long way in improving an all too familiar dismal situation in developing countries. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10045t1.jpg] [cn10045t2.jpg] [cn10045t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}