 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
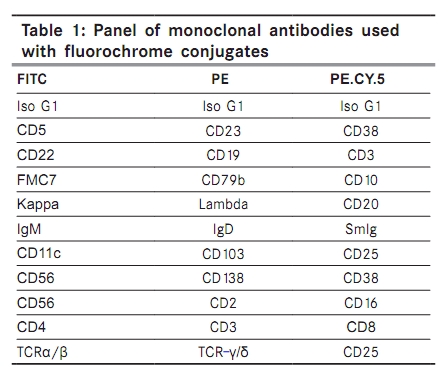
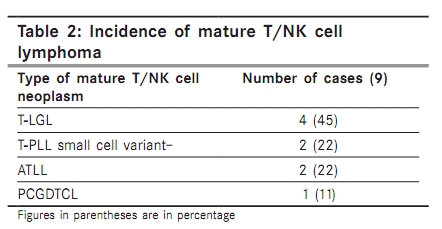
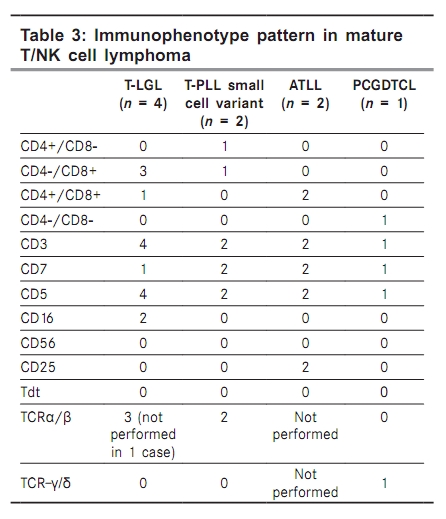
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 189-193 Original Article Immunophenotyping of mature T/NK cell neoplasm presenting as leukemia Gujral S, Polampalli S, Badrinath Y, Kumar A, Subramanian PG, Nair R1, Sengar M1, Nair C1 Departments of Pathology and 1 Medical Oncology, Tata Memorial Hospital, Mumbai, India Correspondence Address: Dr. Sumeet Gujral, Department of Pathology, Tata Memorial Hospital, Mumbai, India s_gujral@hotmail.com Code Number: cn10046 PMID: 20448385 DOI: 10.4103/0019-509X.63020 Abstract Introduction : Mature T/NK cell lymphomas (MTNKL) presenting as leukemia are rare and show considerable overlapping of clinical, morphological and immunophenotypic features. Keywords: Flow cytometry, immunophenotyping, mature T/NK cell lymphoma Introduction Mature lymphomas as well as chronic lymphoid leukemia are commonly of the B-cell phenotype. [1] T and NK cell lymphoma/leukemias have many similar clinical and laboratory characteristics due to their origin from a common T/NK cell precursor. There are approximately 18 subtypes of mature T/NK cell neoplasms constituting 12-15% of lymphoid malignancies diagnosed in western countries. [1],[2] Nodal mature T/NK cell lymphomas (MTNKL) are uncommon and MTNKL presenting as leukemia are extremely rare. [3] MTNKL have overlapping clinical, morphological and immunophenotypic features. [4],[5] This overlapping of immunophenotypic overlap may be due to unavailability of specific markers for these tumors. As per various guidelines for panel selection, most of the immunophenotypic panels are B-lymphocyte centric which may be one of the causes of underreporting of MTNKL. [6],[7],[8],[9],[10],[11] Common MTNKL subtypes that present as leukemia include sezary syndrome/mycosis fungoides, large granular lymphocyte leukemia (T-LGL), peripheral T-cell leukemia/lymphoma unspecified (PTCL), adult T-cell leukemia/lymphoma [human T-cell lymphoma/leukemia virus-l (HTLV-1) associated] and T-cell prolymphocytic leukemia (T-PLL). [12],[13] There is a paucity of data of MTNKL cases presenting as leukemia. Aims To illustrate the spectrum of subtypes of MTNKL presenting as leukemia. Materials and Methods We analyzed 410 consecutive samples [bone marrow (BM) and peripheral blood (PB)] of mature lymphoid neoplasm presenting as leukemia over a 4-year period (between 2003 and 2007). All BM aspirate/peripheral blood PB smears were air dried and subsequently stained with Wright′s stain. These cases were diagnosed based on immunophenotyping of PB and BM aspirates [Table - 1]. Thirty out of these were follow-up cases and were excluded from the study. Of the remaining 380 cases, there were 356 cases of MBNHL, 12 cases of plasma cell disorders, three cases of Burkitt′s lymphoma and nine cases of MTNKL. The morphology and immunophenotyping data were correlated to classify them as per WHO guidelines. [1] Correlation was carried out with additional materials such as BM, lymph node and skin biopsies, wherever available. Immunohistochemistry was performed with additional markers such as CD30, Alk-1 and CD5. Serology was available for HTLV-1 in one case. There were three other cases of anaplastic large cell lymphoma (ALCL) on chemotherapy, which relapsed as leukemia and end-stage disease. These cases were not included. Immunophenotyping PB smear and/or BM aspirates collected in the hospital operation theatre were immediately transported to the flow cytometry (FCM) laboratory. The primary panel included CD19, CD5, CD23, CD20, CD38, CD10, SmIg, FMC7, CD22, CD79b, kappa, lambda and CD3. Additional markers (secondary panel) were analyzed when the primary minimal panel did not yield sufficient marker expression for a diagnosis and included CD4, CD8, CD25, CD16, CD56, CD2, CD7, CD11c, CD25 and CD103. Anti-TCRα/β and TCR γ/δ expression levels could be assessed in a subset of cases only. Tdt was performed in all nine cases. Surface antigens were performed before processing the cells for cytoplasmic and nuclear antigens. An antigen was considered positive based on the antigenic intensity and the percentage positivity of the gated cells (> 20% of the gated cells). [14] Molecular cytogenetic study data are not included as they were available in a few selected cases. Results Of the total of 380 cases of mature lymphoid neoplasm presenting as leukemia, only nine were labelled as MTNKL. These included T-LGL (4), T-PLL small cell variant (2), ATLL (2) and PCGDTCL (1) [Table - 2]. Age ranged from 38 to 70 years with a median age of 56 years. The male to female ratio was 3:1. Cases of T-LGL showed presence of large atypical lymphocytes with moderate cytoplasm and presence of coarse granules. Both cases of T-PLL small cell variant revealed small lymphocytes with scanty cytoplasm, cytoplasmic blebs, dense nuclear chromatin and a small nucleolus. Both cases of ATLL showed intermediate to large-sized atypical lymphoid cells with irregular flowery type nucleus and moderate amount of bluish cytoplasm. The single case of PCGDTCL showed small to intermediate-sized atypical lymphoid cells with a moderate amount of cytoplasm and round to cleaved nucleus with coarse chromatin. There were different expression patterns of different T cell markers in various subtypes [Table - 3]. Three cases of T-LGL revealed CD4-/CD8+ phenotype, while one showed CD4+/CD8+ phenotype. Only two cases expressed CD16. CD3 and CD5 were expressed in all the cases. CD7 was expressed in all except three cases of T-LGL. CD25 was distinctly expressed in both the ATLL cases. T-LGL revealed CD4-/CD8+ phenotype in three and CD4+/CD8+ phenotype in one case. CD56 was absent in all the cases of T-LGL. One case of T-PLL small cell variant showed CD4+/CD8- phenotype, while the other case showed CD4-/CD8+ phenotype. Both cases of ATLL showed CD4+/CD8+/CD25+ phenotype. The single case of PCGDTCL showed a CD4-/CD8- phenotype pattern. TCRα/β was seen in three cases of T-LGL, while in could not be performed in one case. TCRα/β was also seen in both the cases of T-cell PLL small cell variant. TCR γ/δ was seen in only one case of PCGDTCL. Tdt was negative in all these cases. BM trephine biopsy revealed diffuse and interstitial infiltration of atypical lymphoid cells in all cases. Lymph node biopsy was available and correlated in cases of ATLL and T-PLL small cell variant, whereas the single case of PCGDTCL had skin biopsy confirmation. Immunohistochemistry findings correlated well with the FCM findings. Discussion Nodal mature T/NK cell lymphomas constitute 10% of all the NHL in India, [15] an incident as reported in the west. [16] However T-cell lymphoblastic lymphomas are common in India like in the rest of the eastern countries. [15] There is a paucity of literature on MTNKL presenting as leukemia. [3],[17],[18] T/NK cell lymphomas rarely present as leukemia. MTNKL constituted 4% of all the mature lymphoid neoplasms presenting as leukemia at our center, similar incidence as reported. [3] Classically included in this group are sezary syndrome/mycosis fungoides, LGL, PTCL, ATLL and T-PLL. [12] We had four cases of T-LGL, two of T-PLL small cell variant, two of ATLL and one of PCGDTCL. T-LGL was the most common subtype of MTNKLs, as reported elsewhere. [1] This is in contrast to nodal MTNKL, where common subtypes at our center include ALCL of T/null-cell type (4.3%) and other nodal peripheral T-cell lymphomas (2.9%). [15] T-cell lymphoblastic lymphoma (T-LL) (6%) is the most common subtype of T-cell malignancies. [15] T-LGL is usually defined as an indolent lymphoproliferative disorder composed of lymphocytes with cytoplasmic cytotoxic granules. The classic immunophenotype of T-LGL is CD3+/CD4-/CD8+/CD16+/CD57+. [19],[20] Occasional case reports have described CD4+/CD8- T-LGL leukemias, [21] dual-positive CD4+/CD8+ T-LGL leukemia [22] and dual-negative CD4-/CD8- cases. [19] CD56 expression is associated with a more aggressive clinical course. [23],[24] CD56 was negative in all cases. Expression of NK related antigens CD16 (~80%) and CD57 (approximately 100%) along with granzyme B and TIA-1 is usual in T-LGL leukemia. [25],[26] Expression of CD57, granzyme B and TIA-1 could not be evaluated. TCR α/β was expressed in all three cases of T-LGL. In the vast majority of cases reported in the literature, the TCR is of the α/β subtype [19] and rarely of the TCR γ/δ subtype. [19],[27] Classically the lymphoid cells of T-PLL have a characteristic prolymphocyte morphology with tumor cells being intermediate in size, low nuclear/cytoplasmic ratio, moderately condensed chromatin and, as a hallmark, a single, prominent central nucleolus. [28],[29] However 20% of T-PLL cases are termed the "small cell variant," of T-PLL in which the nucleolus is not obvious by light microscopy and is visible only by electron microscopy. [28],[29] Both our cases of T-PLL were of this subtype, one with CD4+/CD8- phenotype [30] and the other with CD4-/CD8+ phenotype, as reported elsewhere. [29] Both revealed a TCR α/β immunophenotype. ATLL reveals presence of abnormal T lymphocytes with indented or lobulated nuclei, suggesting the term flower cells. Both cases of ATLL showed similar morphology and expressed CD4+/CD8+/CD25+ phenotype. T-cell-associated antigens such as CD3, CD5 and CD7 are variably expressed on immunophenotypic analysis, although one of the mature T-cell antigens (CD5 or CD7) is usually lost. Furthermore, CD4 is more commonly expressed than CD8. [31] However both our cases expressed CD7, CD5, CD4 and CD8. Although hepatosplenic γ/δ T-cell lymphoma is the prototypic γ/δ T-cell neoplasm, cutaneous γ/δ T-cell lymphoma and γ/δ T-cell LGL leukemia have also been described. [1],[27],[32] Tumor cells in our single case of PCGDTCL expressed CD3, CD7, CD5 and TCR γ/δ. However, they were negative for CD4 and CD8. Occasional published reports of PCGDTCL presenting as leukemia reveal expression of CD2, CD3 and CD56 and negative for CD4, CD8, CD5 and CD7. [32] There were a few drawbacks of this study. We did not include staging BM for immunophenotyping. FSC/SSC gating was performed for all cases. There were 13-20 antibodies used for immunophenotyping (mean = 15). Our primary panel for mature lymphoid neoplasms is B-cell centric with only two T-cell markers (CD3 and CD5). CD4 and CD8 were carried out in selected cases only with a suspicion of T-cell lymphoma. Our panel did not include antibodies like CD43, CD57, TIA-1, granzyme B, CD30 and CD52. TCRα/β, TCR γ/δ and CD56 was included in few cases only. Correlation with complete blood counts and clinical and treatment follow-up was not performed. Molecular studies were not carried out. Few of our cases of hepatosplenic gamma delta T-cell lymphoma might have been mislabelled as T-cell acute lymphoblastic leukemia in the past owing to ignorance and also the absence of markers like Tdt, TCR α/β and TCR γ/δ in the primary panel. Conclusion It is often more difficult to identify phenotypically abnormal T or NK cells than abnormal mature B cells by FCM. In addition, the classification of T- and NK-cell neoplasms is less well established than that of B-cell neoplasms, and often requires assimilation of information from multiple sources. Nodal MTNKLs constitute approximately 10% of all NHLs, while MTNKL constitute 4% of all mature lymphoid neoplasms presenting as leukemia in India. T-LGL is the most common subtype. We conclude that flow cytometric features that are most suspicious for a MTNKL include loss of CD7, while CD3 and CD5 are expressed in most cases. Low incidence of MTNKL may be a true representative of its incidence or else may be due to selection bias as staging BM were not immunophenotyped. Immunophenotyping of mature hematolymphoid neoplasms with a limited number of antibodies will not help in the diagnosis of MTNKL with certainty, as there is an overlap between the immunophenotypic profiles of different subtypes. Immunophenotypic character of each subtype reveals that there is lack of complete faithfulness of any one immunophenotype for a particular MTNKL subtype. List of reagents of clinical utility in the evaluation of MTNKL neoplasms include CD2, CD3 (surface), CD4, CD5, CD7, CD8, CD45, CD56, CD1a, CD3 (cytoplasmic), CD10, CD16, CD25, CD26, CD30, CD45RA, CD45RO, CD57, TCRα/β, TCRγ/δ, TIA1, T-β chain isoforms. [33] Immunophenotypic profile has to be interpreted in conjunction with morphology to diagnose such cases. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10046t1.jpg] [cn10046t3.jpg] [cn10046t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}