 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 199-205 Original Article Assessment of perineural infiltration and spread of oral squamous cell carcinoma: A clinicohistopathologic study Agni NA, Prasad GSV, Borle RM, Shukla S1, Grover S1, Korde S1 Departments of Oral and MaxilloFacial Surgery and 1 Pathology, Sharad Pawar Dental College, Sawangi (Meghe), Wardha, Maharashtra, India Correspondence Address: Dr. Nisheet A Agni, Department of Oral and MaxilloFacial Surgery, Sharad Pawar Dental College, Sawangi (Meghe), Wardha, Maharashtra nisheetagni@yahoo.com Code Number: cn10048 PMID: 20448387 DOI: 10.4103/0019-509X.63024 Abstract Background : As the tumor spreads through the pathway of least resistance, the present study was carried out to evaluate the presence of perineural infiltration and spread of oral squamous cell carcinoma (OSCC) along the perineural spaces in gingivobuccal sulcus tumors infiltrating into the mandible.AIMS and objectives : (1) To investigate the incidence of perineural invasion of OSCC along the inferior alveolar nerve and (2) to investigate the neurovascular bundle as a potential route of spread of OSCC. Materials and Methods : Twenty-six patients with histopathologically proven OSCC of the gingivobuccal sulcus with radiographic infiltration of the mandible were included. The surgical specimens were decalcified and serially sectioned. Each section was stained with hematoxylin and eosin and was screened for the presence of perineural invasion and spread. Results : Twenty-five specimens showed perineural infiltration but none of the cases showed perineural spread along the inferior alveolar canal. Also, not all cases showed any neurologic deficit. Follow-up of these cases showed early recurrence (6-8 months) in the study group. Conclusion : Perineural infiltration is present in OSCC but perineural spread along the inferior alveolar canal is absent. It is a bad prognostic indicator. Keywords: Endoneural infiltration, neurologic deficit, perineural infiltration, perineural spread, radiographic invasion Introduction Oral cancer accounts for about 4% of all cancers and about 2% of cancer deaths worldwide. In the United States, Europe and Australia, it accounts for 0.6-5% of all cancers, but it accounts for up to 30-50% of all cancers in India. [1],[2] Spread of oral squamous cell carcinoma (OSCC) is dominated by local infiltration and metastasis to regional lymph nodes via the lymphatics. Mandibular invasion by OSCC may progress by either an infiltrative or an erosive or a mixed histological pattern. [3] In case of the former, there is an increased incidence of infiltration of the inferior alveolar nerve. Although the inferior alveolar canal once breached does offer a pathway of least resistance for the tumor to spread, perineural spread of malignancy is not a routine feature of OSCC but is more commonly associated with tumors like adenoid cystic carcinoma. Lesions involving the alveolus in various degrees are treated by segmental resection to resection with disarticulation. The resection is routinely based on clinical and radiological infiltration of the alveolar bone with a safe margin of 1-1.5 cm. Marginal resection is indicated in lesions with an erosive or expansive bony involvement whereas it is not appropriate in an infiltrative type of bone invasion. [4] Hence, it is essential to study whether OSCC spreads along the perineural spaces up to the safe margins of the resection. Evidence of tumor cells in and around the inferior alveolar canal at the so-called safe margins of resection would be instrumental in changing the current concept of locoregional spread, which would then warrant a more radical resection to reduce the incidence of recurrences. Hence, this study was conducted to investigate the incidence of perineural invasion of OSCC along the inferior alveolar nerve and to investigate the neurovascular bundle as a potential route of spread of OSCC. Materials and Methods Twenty-six patients with histopathologically diagnosed OSCC involving the mandibular gingivobuccal sulcus and found fit to undergo surgery, admitted to this hospital in the Department of Oral and Maxillofacial Surgery from 2006 to 2007, were included in this study irrespective of their age, sex, religion and caste. Only lesions with radiographic invasion of the mandibular bone on panoramic radiography were included in the study. Patients with a recurrent lesion or distant metastasis or who underwent prior radiotherapy were excluded from the study. The patients were thoroughly assessed clinically and radiographically. Extension of the lesion onto the lingual side was recorded along with the dental status at the site of the lesion. The neurologic examination at the site of distribution of the inferior alveolar nerve was carried out both objectively and subjectively. The objective assessment was performed by blindfolding the patient and using light touch and firm strokes extraorally on the lower third of the face on the side of the lesion to elicit the presence or absence of superficial and deep sensations. Two-point discrimination was also used. Intraorally, sensory testing was carried out objectively on the gingiva by instrumentation using a moon′s probe. The patients were evaluated radiographically using an Orthopantomogram for diagnosis of bony infiltration of the mandible, which was said to be present if there was presence of the following radiographic features:
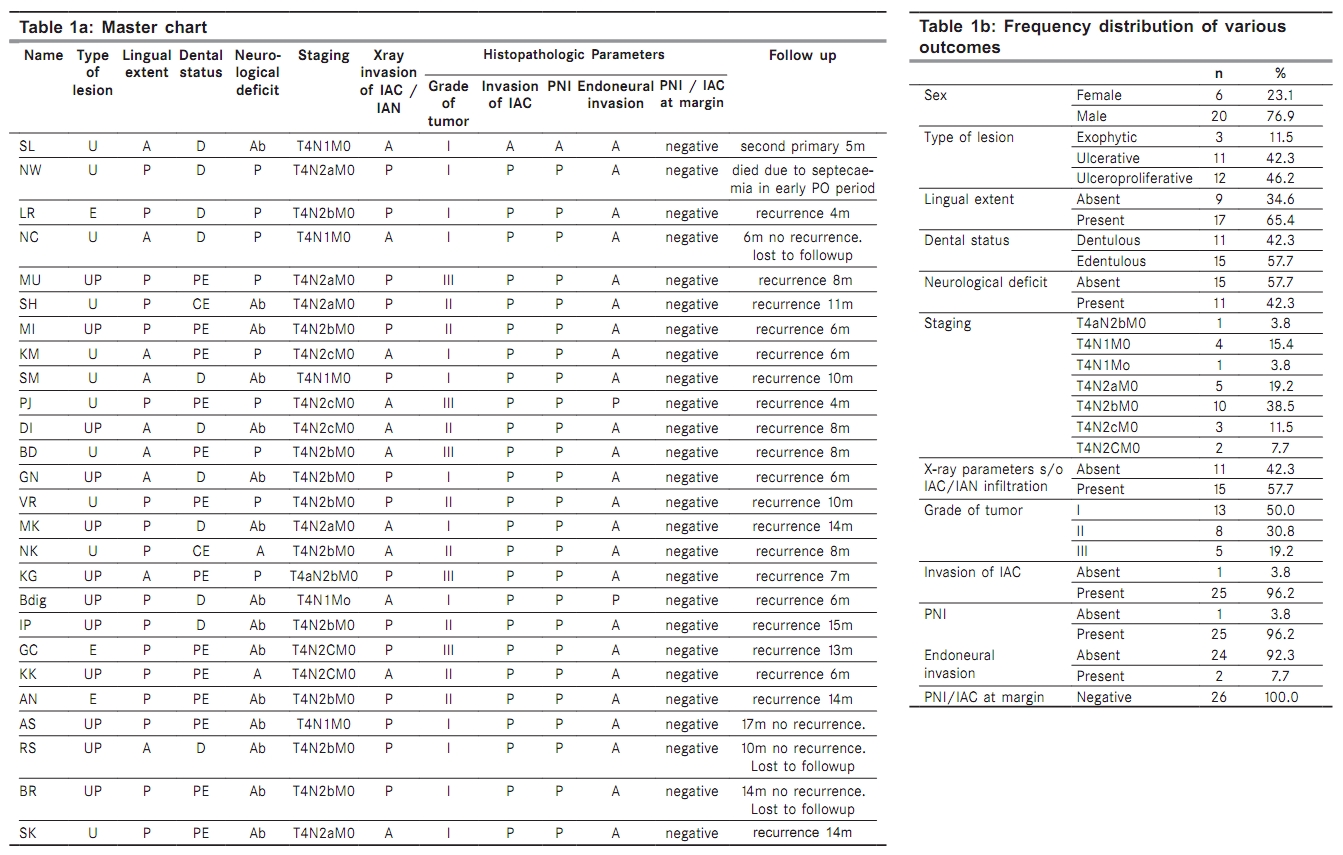
Grade I: well-differentiated SCCs Grade II: moderately differentiated SCCs Grade III: poorly differentiated SCCs All the cases were operated under general anesthesia using the standard surgical protocol. Wide local excision of the lesion with a clear margin of 1.5 cm from the radiologic tumor margins was carried out. The neck nodes were managed by performing a suitable neck dissection depending on the nodal status in a given patient. Intraoperatively, frozen sections were used to ascertain adequacy of excision of soft tissue margins and a radiograph of the excised specimen was taken to ensure that the margins of excision were in the healthy bone. Histopathological techniques The surgically excised specimen was washed under running tap water and immediately fixed in 10% formalin by immersing the entire specimen. The specimen was then decalcified using freshly prepared aqueous solution of 5% nitric acid that was replenished every 24 h. Physical method (needle prick) was used to confirm adequate decalcification of the specimen taking care to use it away from the site of interest to avoid artifacts. The specimens were rinsed under flowing tap water to wash away the acid. The decalcified specimen was then sectioned serially at an interval of 1 cm so that the most distal and proximal section was at least 1 cm beyond the radiological margins of the tumor. The sections were then processed and embedded in paraffin blocks. Routine histopathological processing was carried out to prepare the slides for evaluation. The slides were viewed under a light microscope under low (10X) and high (40X) power to confirm infiltration of malignant cells in the inferior alveolar canal and the perineural area of the inferior alveolar nerve in all the sections. Malignant infiltration into the canal was said to be positive if destruction of the canal walls by malignant cells was evident in the section. If the malignant cells were seen abutting the nerve, it was labeled as perineural infiltration. If the nerve anatomy was distorted due to infiltration of the malignant cells, it was labeled as endoneural infiltration. A single senior pathologist examined all serial sections under the microscope. If tumor cells were seen in the perineural spaces or canal in continuity with malignant cells in the surrounding osseous tissue, it was labeled as "Direct spread." The spread of tumor along the canal or perineural space was considered positive if malignant cells were observed in the perineural space of the inferior alveolar nerve or inferior alveolar canal without an evidence of direct invasion of the tumor cells from the surrounding bone in any of the sections. Results The data was computerized and statistical analysis was performed using a statistical package SPSS. Appropriate statistical tests were applied to test the significance of the results. Descriptive statistics were estimated for quantitative variables. Chi-square test was applied to test the significant differences between the different classes having different frequency distributions. An exact test that does not rely on using the approximate c2 distribution is Fisher′s exact test, which is significantly more accurate in evaluating the significance level of the test, especially with small numbers of observation, and hence was used in the present study. The collected data were organized in a systematic manner and a master chart was formulated [Table - 1]a. Similarly, a frequency distribution table of various outcomes was also formulated [Table - 1]b. Twenty-six patients (20 [76.92%] males and six [23.08%] females) of clinical stage IV and histopathologically diagnosed OSCC of the gingivobuccal sulcus were considered in this study. Their age ranged from 39 years to 70 years, the mean age being 55.84 years (SD 7.94). The mean age of males was 55.7 years (SD 8.11) and of females was 56.33 years (SD 8.04). Three (11.53%) patients showed exophytic growths whereas ulcerative and ulceroproliferative growths were seen in a near-equal number of patients, i.e. 11 (42.30%) and 12 (46.17%), respectively. Fifteen patients (57.69%) were edentulous in the area of the lesion, of which 12 (80%) had visible lingual extent of tumor whereas only five (45.5%) of the 11 dentate patients had a lingual extension of the tumor. Correlation of dental status with lingual extension of malignancy was estimated using chi-square estimate, and it was found that they are not independent of each other because no significant difference was observed (c2 = 3.346, df = 1, Sig. [two-sided] = 0.103) between edentulous and dentate patients [Table - 2], with respect to lingual extension of the tumor. Thus, it can be inferred that spread of malignancy to the lingual side from the gingivobuccal sulcus lesions is not influenced by the presence or absence of teeth. Moreover, we found that 17 lesions showed evidence of invasion of the lingual cortex and thus infiltrated from both the buccal and the lingual direction as compared to nine lesions that showed buccal infiltration alone. Of the 17 specimens with lingual cortical involvement, perineural infiltration was present in all specimens. However, one of the nine specimens that showed buccal infiltration alone did not show pathologic involvement of the perineural spaces. Thus, perineural invasion does not show any site specificity. Panoramic radiographic examination of the patients revealed only 15 (57.69%) patients with radiographically detectable invasion into the mandibular canal. However, 25 (96.15%) patients showed pathologic infiltration of the inferior alveolar canal and nerve. A nonsignificant P-value (0.42) was observed, which is highly suggestive of the inadequacy of plain radiographs to diagnose perineural invasion of OSCC [Table - 3]. All 26 (100%) patients reported with a chief complaint of pain, whereas 11 (42.31%) patients showed clinical signs of sensory deficit in the distribution of the inferior alveolar nerve, which included paresthesia or anesthesia. However, 25 (96.15%) specimens showed histopathologic involvement of the perineural spaces of the Inferior alveolar nerve and two (7.70%) specimens showed endoneural invasion. The inference that can be drawn is that pain in case of OSCC lesions of the gingivobuccal sulcus is not related to presence or absence of perineural invasion or spread (P > 0.05). Also, perineural invasion by OSCC does not always manifest as neurologic deficit, although the vice versa may be true [Table - 4]. Correlation between evidence of perineural invasion with clinical symptoms and signs of neurological deficit suggested that of the 25 patients with histopathologic proof of perineural invasion, only 11 patients had clinical evidence of neurological deficit. Fourteen patients without clinical evidence of nerve involvement had demonstrable perineural invasion. Because the Fisher exact sig P-value (1.0) was found to be statistically insignificant, it can thus be inferred that neurologic deficit, although suggestive of perineural infiltration of the inferior alveolar nerve, is not always manifested until the lesion is advanced. Distribution of lesions according to Brooder′s histopathologic grading was 13 cases (50%) of Grade I, eight cases (30.76%) of Grade II and five cases (19.24%) of Grade III lesions. Also, histopathologic grade of the tumor does not influence invasiveness of the lesion and might not influence perineural invasion of the inferior alveolar nerve. Follow-up of these patients suggested an early recurrence in most of the cases, ranging from as early as 4 months postop to 14 months postop. Only one patient showed no recurrence for 17 months and is currently under follow-up. Three other patients showed no recurrence for 6, 10 and 14 months, respectively, in the postoperative period, but were lost to follow-up after the specified period. One patient died of sepsis in the immediate postoperative period. The only patient who did not show perineural invasion developed a second primary lesion within 5 months. Patients with recurrence were either advised second surgery or referred for chemoradiotherapy, depending on the case. However, none of the patients agreed for a second surgical procedure due to their financial constraints and were lost to follow-up. Hence, their survival could not be recorded. Discussion The spread of OSCC mainly occurs through local invasion and spread via local lymphatics into the draining lymph nodes. Spread via the hematogenous route by formation of embolus is a feature of advanced disease. Perineural spread of malignancy is not a routine feature of OSCC but is more commonly associated with tumors like adenoid cystic carcinoma. Hence, current management protocols for OSCC involving the gingivobuccal sulcus consider only local and regional spread of the tumor. If the lesion extends both buccally as well as lingually, infiltration of the bone and perineural spaces is much faster. The cortical bone being stronger provides more resistance to infiltration as compared with the cancellous bone, which has more marrow spaces and is less dense. However, the edentulous mandible has cortical defects that result in a faster spread of the malignant cells into the cancellous bone and thus into the inferior alveolar canal. In our study, 17 cases with lingual extension showed gross invasion of the mandibular bone, with a few cases showing pathologic fracture and all cases showing pathologic invasion of the perineural tissues. These findings corroborate with the findings of McGregor et al. (1987), who suggested that there is continuity between the inferior alveolar canal and the overlying mucoperiosteum in an edentulous mandible. [5] The study by Totsuka et al.(1991) also showed that the rate of spread of OSCC is unimpeded in the cancellous bone than in the cortical bone. [6] Pain in OSCC is a result of secondary infection in the lesion, which undergoes repeated trauma and irritation of the nerve endings, whereas neurological deficit denotes perineural invasion. Eleven patients showed clinical signs of neurosensory deficit in the distribution of the inferior alveolar nerve. However, 25 specimens showed histopathologic involvement of the perineural spaces of the inferior alveolar nerve and two specimens showed endoneural invasion. This suggests that absence of neurosensory deficit does not exclude the possibility of malignant infiltration of the inferior alveolar nerve. The nerve fibers are themselves usually intact due to distensibility of the perineural and endoneural spaces and undergo pressure degeneration only in later stages of the disease in confined spaces, as suggested by Dodd et al. (1970). [7] Thus, neural involvement extensive enough to cause transmission blockage is not common. Carter et al. (1982), in their study, found congruence in the clinical and pathological evidence of nerve involvement in about two-third of the cases. [8] Our results are in support of Carter′s findings. Fifteen of the 25 specimens with perineural invasion had radiographically detectable invasion into the mandibular canal. This finding corroborates with that of Totsuka et al. (1991), who found that comparison between radiologically predicted extent of bone defect and histopathologic extent is highly subjective and not necessarily accurate. [6] Pathologic grading of tumor based on the percentage of abnormal cells in the total cellular elements was considered helpful previously to plan the treatment. Totsuka et al. (1991) suggested that invasion is more in case the tumor has a higher grade. [6] Tuse et al. (1994) observed that well-differentiated tumors invade the bone with a similar propensity as poorly differentiated tumors. [9] In our study, we found that all the grades of lesions showed perineural invasion and Grade I lesions formed 50% of the sample size. Also, endoneural invasion was seen in one Grade III and one Grade I lesion. Only one Grade I lesion showing endoneural invasion had a direct infiltration of malignant cells into the nerve at the mental foramen. Thus, we can say that infiltration of the tumor into the nerve depends on the proximity of tumor cells to the nerve and is by way of local invasion. The grade of the tumor does not play any significant role in the invasion of the nerves. Histopathologic infiltration of the inferior alveolar nerve by the OSCC was seen in 25 of 26 cases in our study. This high incidence was because our selection criteria included only those malignancies that showed radiographic infiltration of the bone on orthopantomogram. This is suggestive of increased risk of perineural involvement in advanced stages of the disease, which is in accordance with the observations of Dodd et al. (1970), who found an increased propensity of neural involvement in advanced and recurrent disease. [6] In our study, all sections of the specimens showed a continuity of malignant cells in the surrounding bone and perineural tissues, which suggested direct infiltration into perineural spaces by the malignant cells. Thus, we found no evidence of perineural spread of OSCC that would warrant an extensive resection beyond the accepted 1.5 cm safe bony margin, which is contrary to Pandey et al., who found a 20% perineural spread of OSCC along the inferior alveolar nerve. [10] However, the malignant cells are known to traverse great distances along perineural spaces, as suggested by Dodd et al. (1970) and McGregor et al. (1986). [5],[7] The shortcomings of our study are that we have not assessed the perineural area beyond the resection margin. Thus, any skip metastasis due to bodily locomotion of the malignant cells along the nerve beyond the resection margins is not examined. Follow-up of these cases suggested an early recurrence in most of the cases, which is suggestive of perineural invasion as a bad prognostic sign, which is in accordance with Soo et al., who suggested that perineural and endoneural infiltration of the inferior alveolar nerve is an adverse prognostic factor for increased locoregional recurrence and decreased survival. [11] Conclusion Perineural invasion results from direct spread of the malignant cells into perineural spaces. Perineural spread of OSCC along the perineural spaces is not seen and does not warrant any change in the surgical protocol. Perineural involvement of OSCC cannot be diagnosed by clinical and radiological means alone. Hence, histological examination of the specimen should be carried out routinely to confirm neural involvement so as to plan any adjuvant therapy to improve locoregional control, as perineural invasion suggests a bad prognosis. Acknowledgments The authors would like to thank Mrs. Hem Sethi, Senior research officer, AIIMS, New Delhi for the statistical analysis. They would also like to thank Dr. (Mrs.) Vagha, Head, Department of General Pathology, JNMC, Wardha, and Dr. Biju Papachan, Ex-Lecturer, Department of OMFS, SPDC, Wardha for their guidance during the study. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10048t2.jpg] [cn10048t1.jpg] [cn10048t3.jpg] [cn10048t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}