 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
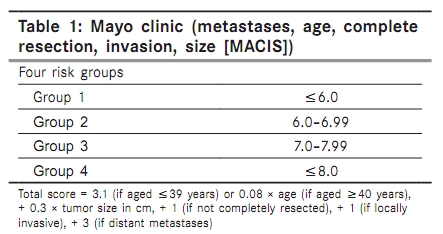
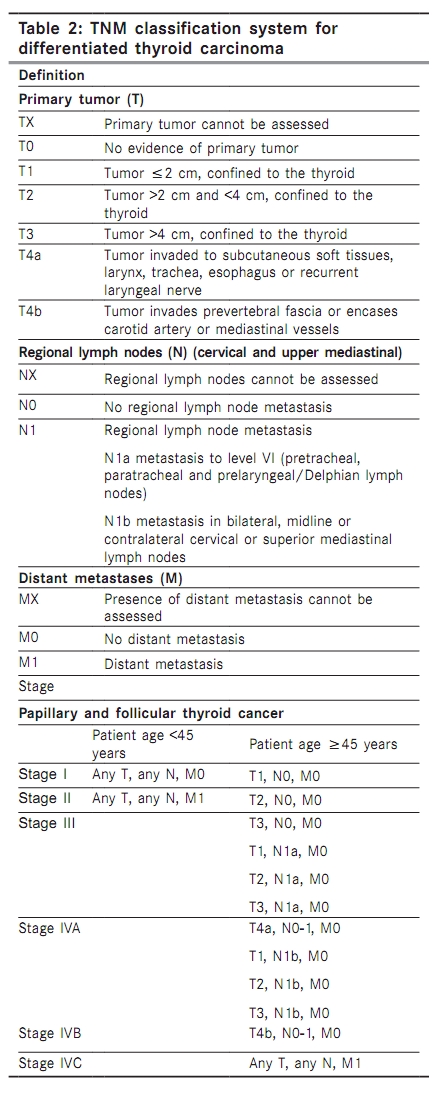
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 206-216 Review Article Papillary thyroid carcinoma: Debate at rest Sonkar AA, Rajamanickam S, Singh D Department of Surgery, Chhatrapathi Shahuji Medical University (Formerly King George's Medical University), Lucknow, UP, India Correspondence Address: Dr. Abhinav Arun Sonkar, Department of Surgery, Chhatrapathi Shahuji Medical University (Formerly King George's Medical University), Lucknow, UP, India vandana_abhinav@rediffmail.com Code Number: cn10049 PMID: 20448388 DOI: 10.4103/0019-509X.63025 Abstract Introduction: Papillary thyroid cancer (PTC) is the most common well-differentiated cancer of the thyroid and is one of the fastest growing group of cancers probably because of the increased use of ultrasound (HRUSG) in the evaluation of the thyroid in recent years.Materials and Methods: A MEDLINE and OVID database search was performed to collect information on papillary thyroid carcinoma. Recently published consensus guidelines were also used as an additional resource. Conclusions: The controversy regarding the extent of thyroidectomy in patients of PTC is relatively settled, with total thyoidectomy being the preferred approach with nodules >1.5 cm in size. Lymph node (LN) metastases do not seem to affect the overall survival, but they do increase the recurrence rate. It is worthwhile to offer LN dissection at initial surgery if LNs are ultrasonologically diagnosed to harbor malignancy. In experts hands, the rate of recurrent laryngeal nerve injury and hypoparathyroidism is negligible in a neck dissection in initial surgery and remains negligible if carried out in a redo or completion scenario. Keywords: Extent of surgery, papillary thyroid cancer, staging Search Strategy The MEDLINE and OVID databases were used to search for information on papillary thyroid carcinoma between 1979 and May 2009. Relevant articles in English with specific interest in papillary thyroid carcinoma were reviewed. References of such articles generated also enabled widening the reference pool. Many of the recently published guidelines from various organizations and their corresponding references were also used as an additional resource and cited wherever appropriate. Introduction Papillary thyroid cancer (PTC) is the most common well-differentiated cancer of the thyroid. It represents approximately 80-85% of well-differentiated thyroid cancers. [1],[2] Thyroid cancer affects women more than men, and the median age of onset is the fourth and the fifth decades of life. PTC is one of the fastest-growing groups of cancers, and this could be due to the increasing use of ultrasound (HRUSG) in the evaluation of the thyroid gland. [2] Well-differentiated cancers of the thyroid gland carry a good prognosis and have good long-term survival rates. Detection of smaller nodules than those diagnosed previously has further enhanced better survival data in the recent past. PTC < 1 cm has been termed papillary thyroid microcarcinoma (PTMC). Risk Factors Radiation exposure is the most well known and most studied risk factor for PTC. [3] PTC following the nuclear fallout in Chernobyl and the survivors of the nuclear bombs in Hiroshima and Nagasaki are well known. Other less-studied risk factors include dietary habits, lifestyle, parity and genetic predisposition. Diagnostic Evaluation of PTC Fine needle aspiration biopsy (FNAB) is the workhorse in evaluation of the thyroid nodule. Its easy availability, simplicity in performance and accuracy in the range of 70-97% in the detection of malignancy have made it the initial investigation in the evaluation of the thyroid nodule. The use of HRUSG and other imaging modalities, like computerized tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET) scan in the assessment of thyroid disease has greatly increased the detection of small thyroid nodules that had gone unrecognized in clinical examination. [4],[5] When examined by HRUSG, rather than by palpation, thyroid nodules are commonly detected with a prevalence of 40-50% in the general population. [6] Although most such thyroid "incidentalomas" are benign, approximately 5-6.5% may be malignant. [7] FNAB yields inadequate diagnostic material in 15-25% and repeat aspiration, especially guided by the HRUSG, can augment the accuracy of the procedure. [8] Although studies seeking to identify features that accurately predict malignancy have given mixed results, there are certain sonographic features that have been consistently associated with malignancy, including hypoechogenicity, increased vascularity, microcalcifications, irregular margins and the absence of a halo. [9] Hypoechoic nodules are associated with malignancy. [10] This appearance is thought to result from the increased cellularity and cellular compaction seen in PTC. In contrast, a follicular neoplasm, whether a benign follicular adenoma or a follicular carcinoma, is composed of small microfollicles with variable amounts of colloid. The echogenicity of follicular carcinomas may depend on the colloid content; more the colloid content, more hyperechoic the lesion. [11] Cystic change is highly characteristic of PTC. Furthermore, cystic lymph nodes (LNs) can also be identified by USG, having a thickened outer wall, internal echoes and nodularity with septations. USG also has the ability to detect microcalcification and nodular vascularity with good inter-observer reliability. [12] The vascularity of a thyroid nodule is demonstrated with color flow Doppler (CFD) or power Doppler (PD) imaging. Increased intranodular flow is associated with malignancy and has good inter-observer variability. Calcifications are present in up to 30% of thyroid nodules. Microcalcifications image as echogenic foci smaller than 2 mm and are associated with malignancy. Microcalcifications are thought to represent aggregates of psammoma bodies, the laminated spherical concretions characteristic of many papillary cancers, and are rarely found in benign nodules or follicular neoplastic lesions. [13] Coarse or dense calcifications are larger than 2 mm and cause posterior acoustic shadowing. These dystrophic calcifications occur in both benign and malignant lesions in areas of fibrosis, tissue degeneration and necrosis. Coarse calcifications may be associated with malignancy when they appear with microcalcifications or in the center of a hypoechoic nodule. [14] Chan et al., in their retrospective study of 55 patients with PTC, determined that the typical appearance of papillary carcinoma is a round, solid, hypoechoic mass with internal vascularity and microcalcifications. Uncommon findings were cystic elements, a hyperechoic texture, intrinsic hypovascularity, sharp angular contours and metastatic spread without a visible thyroid mass. Uncommon sonographic features were found to occur more often that expected. The above-mentioned ultrasonographic characteristics of PTC are not significantly influenced by age, sex or autoimmune thyroiditis. The feature with the greatest inter-observer variability and hence limited utility is the margin of the nodule. [15] None of these characteristics were associated with increased LN metastasis. There are several additional sonographic features of thyroid nodules that have been shown to be associated with malignancy in small studies. The shape of the nodule has been evaluated by looking at the ratio of the anteroposterior to transverse diameter (A/T). When the antero-transverse (A/T) ratio is> 1.0, indicating a spherical nodule, Cappelli and colleagues found that this detected thyroid cancer, with a sensitivity of 84% and a specificity of 82%. [16] A recent study examined tissue stiffness as a risk factor for malignancy in a subset of nodules with indeterminate cytology using a technique called elastography. [17] High elasticity scores, indicating stiffness, were found in patients with malignant histology and low scores in patients with benign lesions. Finally, extrathyroidal invasion may be occasionally seen when the tumor growth extends through either the anterior or posterior thyroid capsule, which normally appears as a bright white outline surrounding the thyroid. In such instances, the margin of the tumor has an ill-defined edge that interrupts this capsule. Considerable debate existed regarding the optimal management of the nonpalpable thyroid nodule, termed the "thyroid incidentaloma." Most reports have shown that incidentally discovered papillary carcinomas of the thyroid gland follow an indolent course. [18],[19],[20],[21] The dimensional cut-off beyond which US-guided FNAB (FNA-US) should be performed has also been a hotly debated issue. Papini et al., in a prospective study of 494 patients with nonpalpable thyroid nodules, confirmed the cost-effectiveness and feasibility of FNA-US of lesions> 8 mm in size or those with at least two features of malignancy. FNA-US restricted to evaluation of nodules> 10 mm in size would have missed 12 of 31 thyroid carcinomas. Nodules smaller than 8 mm with no features of malignancy are better followed with serial US than subjected to unnecessary surgery. [7] There are a few groups who aspirate all nodules regardless of size in the goal to identify PTC. If worrisome aspects apply, even smaller solitary nodules between 5 and 8 mm should be considered for aspiration on an individual basis, based on personal view, patient desires, clinical context and sonographic appearance. [22] Sensitivity for the FNA-US is in the range of 80-90%. [23] Diagnostic accuracy in cystic lesions is low. A combination of FNA-US with thyroglobulin (Tg) assay of the FNAB material increases the accuracy to 90-100% in the above situations. [24] The diagnostic value of serum Tg in washout fluid from the FNAB of the cervical LN metastases from differentiated thyroid carcinoma measurements is maintained despite the presence of circulating anti-Tg antibodies. Preoperative Evaluation of PTC Features specific to PTC, such as multicentricity, increased propensity to lymph nodal metastasis and poor diagnostic accuracy of clinical examination has led to Ultrasound emerge as a valuable tool in the evaluation algorithm prior to surgery. Lymph nodal metastases are seen in up to 80% of PTC patients. Palpation alone is woefully inadequate to judge LN metastasis, missing 40-50% of lymph nodal metastases when compared to HRUSG. [25],[26],[27] Although the rate of detection of micro and macrometastases increases, their role on the overall survival is still questionable. There has been skepticism regarding the routine use of HRUSG in the preoperative setting, as Wang et al., in their prospective study of 508 patients, found that the rate of recurrence was 3% when HRUSG was not performed in the preoperative setting, suggesting little clinical benefit from its use, and preoperative HRUSG would result in the performance of a number of unnecessary extensive procedures to prevent a very few recurrences, notwithstanding the dangers of such recommendations in the hands of inexperienced surgeons. [28] A few small prospective randomized studies studying the above benefit of preoperative HRUSG in the evaluation of PTC patients have shown tendencies toward usefulness of the procedure. Moreover, the morbidity of reexploration, especially of the central compartment in cases of recurrences, has favored the early detection of metastatic disease with the help of HRUSG. [29],[30] Increase in specialist centers adept at neck dissection and the effectiveness of postoperative radioiodine ablation also support its use. The role of CT scan in the evaluation of LN metastasis in the preoperative setting has been studied. Kim et al. also compared HRUSG alone, CT alone and combined HRUSG and CT in the detection of metastases and found that the HRUSG/CT combination was found to be superior to HRUSG alone for the detection of metastatic LNs in the lateral neck levels in PTC patients by level-by-level analysis. However, routine use of the combination has yet to be substantiated. [31] Patterns of LN Metastasis Although LN metastasis does not affect the overall survival, better locoregional control and disease-free survival can be obtained with cervical lymphadenectomy. Lymphatic metastasis develops in approximately 30-80% of patients with PTC. [32],[33],[34] It has been established that regional metastasis is most common to the central compartment of LNs. [35] The rate of level 6 metastases may be as high as 50-65%. [36],[37] White et al. describe the spread of malignant thyroid tumor cells as flowing through the lymphatic system in a sequential fashion from the thyroid gland to the central compartment to ipsilateral compartments and to contralateral and mediastinal compartments. [38] Whereas the involvement of the central compartment nodes is straight forward, knowledge on the patterns of metastasis to the lateral LN groups are now being discussed. Level 3 LNs are the most commonly involved group in the lateral group of LNs. Knowledge of the patterns of metastasis is important in selection of appropriate surgical resection for nodal metastasis. [39],[40] Staging Although the prognosis of PTC is generally good, up to 10% of the patients would eventually die of the disease and an even greater proportion would face the morbidity of recurrences. As a result, a number of studies have identified various clinicopathologic predictors for PTC and devised risk-group stratification or staging systems to select those at high risk of cancer death for more aggressive surgical and adjuvant treatment while those at low risk would be spared of aggressive treatment. This is known as the stage-specific treatment. Some of the staging modules have been depicted in the table below. Given the number of staging systems described in the literature, several studies have attempted to compare the predictability of these staging systems in different populations. A large study conducted by Lang et al. comparing 14 staging systems showed that the three highest-ranked staging systems were the metastases, age, completeness of resection, invasion, size (MACIS) by the Mayo Clinic [Table - 1] followed by the new AJCC/UICC 6th edition tumor, node, metastases (TNM) [Table - 2] and the European Organization for Research and Treatment of Cancer (EORTC). [41],[42],[43],[44] All of the currently staging systems fared well with PTC, regardless of which histologic type they were derived from. When predictability was measured, the MACIS system was the most predictive staging system and so could be the staging system of choice for PTC in the future. Extent of Surgery The ideal surgical procedure for PTC has been a debate for decades. Important questions have been answered by recent studies but still certain grey areas remain. The extent of thyroid resection could vary from lobectomy to near-total thyroidectomy, and the presently preferred total thyroidectomy. [45] The presence of LN metastasis in the central compartment in 50-70% of patients with PTC has led to some centers combining total thyroidectomy with prophylactic level 6 LN dissection. For most patients with thyroid cancer, near-total or total thyroidectomy is recommended if primary carcinoma is more than 1-1.5 cm. Earlier studies on survival data in patients being operated for PTC showed a survival difference of total thyroidectomy over lobectomy in tumors> 3 cm. A recent large retrospective study by Bilimoria et al. [46] of 15,173 patients showed for the first time that lobectomy for lesions between 1 and 2 cm resulted in a higher risk of recurrence and death. Even in lesions < 1-1.5 cm, near-total or total thyroidectomy is offered if they belong to a high-risk group. Older patients more than 45 years may also be recommended near-total or total thyroidectomy because of higher recurrence rates in this age group. [42],[46],[47],[48],[49],[50] Increased extent of primary surgery may improve survival for high-risk patients, while rates of recurrences are reduced by total or near-total thyroidectomy even among low-risk patients. [51],[52],[53],[54],[55] At the same time, a study by Alvarado et al. showed that the complications rates were similar in total thyroidectomy with central lymph node dissection (CLND) compared to CLND subsequent to total thyroidectomy. In their study, 170 (M/F: 28/142) patients (Grp A) had a CLND as part of their primary surgical procedure while 23 (M/F: 10/13) patients (Grp B) underwent CLND as a secondary procedure (12 therapeutic/11 prophylactic procedures). The incidence of temporary hypocalcaemia was 12% vs. 9%, permanent hypoparathyroidism was 1.8% vs. 0%, temporary recurrent laryngeal nerve (RLN) paresis was 3% vs. 4% and permanent RLN paresis (0.6% vs. 0%). [56] The recommendations of the American Thyroid Association Guidelines Task Force are now standard of care in the management of PTC. [25] The surgical management has shifted from subtotal to total thyroidectomy in the management of benign multinodular goiter, where total thyroidectomy may become the procedure of choice for malignant nodules of any size in the near future. [57] PTMC Increasing use of investigations, especially the HRUSG, has permitted the FNAB of lesions as small as 3 mm in size. Papillary neoplasms that are 10 mm and less are considered PTMC. The management of PTMC is controversial as the same principles of treatment of PTC would be too aggressive an approach for the former and the paucity of epidemiological information has led to the widespread variation in management of such lesions from simple observation to total thyroidectomy. [58],[59],[60] The important aspect in the management of PTMC is the establishment of multifocal disease, which would warrant total thyroidectomy and radioiodine ablation. [61] The use of radioiodine as additional treatment following total thyroidectomy, however, has been questioned as more than 99% of PTMC patients are not at risk of distant spread or cancer mortality. [62] Less-aggressive approaches using thyroid lobectomy for unifocal disease seems to be appropriate; however, large studies are required to determine proper management protocols for this "epidemic of microcarcinomas." [63] Treatment of Nodal Metastasis The regional LN metastases are present at the time of diagnosis in 20-90% of patients with papillary carcinoma and a lesser proportion of patients with other histotypes. [57] In a communication to Stulak, Dr. Quan Yang Duh quoted a Japanese study, which stated that in cases of PTC two-thirds of the time the central neck has positive LNs, in ipsilateral neck in two-thirds of the patients, in the contralateral neck in one-third and in mediastinum in one-third of the patients. [27],[64] This widespread LN involvement can be found even in very low-risk micro PTC. In contrast, clinically significant cervical LN recurrence occurs in only 20-30% of the patients. Thus, most LN metastases remain dormant and do not become clinically significant. However, it is difficult to determine which of the positive LN are likely to manifest as malignancy later. [65] In a landmark study of 1,355 patients by Mazzaferri et al., a multivariate analysis of these patients found that the presence of cervical LN metastasis was a significant prognostic factor for the recurrence of disease. [34] The LN involvement is part of the primary disease itself and therefore the aim of the surgeon should be to include a LN dissection to complement total thyroidectomy. [64] A number of studies have shown improved outcome with formal LN dissection with a reduced recurrence rate. True soft tissue recurrences are less as compared to LN recurrence. Neck dissection for LN reduces the relapse of the disease and provides for a higher disease-free survival. This also reduces the need for overall radioiodine therapeutic dose and the risk of dedifferentiation of recurrent tumor to the anaplastic type in patients with a long-term and near-normal life span. [66] The American Thyroid Association recommends routine level 6 LN dissection along with total thyroidectomy even in the absence of clinical or radiological nodes. [25] The rationale for this comes from studies showing that regional LN metastases are present to up to 20-90% at the time of diagnosis even when they clinically or radiologically appear normal. Moreover, level 6 lymph nodal clearance enables a more thorough clearance of all thyroid tissue. Less debate exists when LNs are detected prior to surgery. Sywak et al. showed that routine ipsilateral level 6 LN dissection reduced serum Tg levels compared to total thyroidectomy alone, signifying better thyroid tissue clearance albeit with a minimal increase in the feared complications of permanent hypocalcaemia or recurrent laryngeal nerve palsy. [67] A lateral neck dissection (levels 2, 3 and 4) is warranted when locoregional lymph nodal metastasis is present. Radioiodine "Ablation" is the first-time administration of 131 I to a patient with well-differentiated thyroid cancer. This is typically within 4-8 weeks after the patient′s initial diagnosis and thyroidectomy. Radioactive iodine is taken up by the residual thyroid tissue, and decays releasing beta rays that destroy the cell. Even after total thyroidectomy, some thyroid tissue usually remains, and the primary objective of ablation is to destroy this normal residual thyroid tissue. "Treatment" is the term applied to the administration of 131 I for recurrent or metastatic cancer. [68] Radioiodine as an adjuvant therapy following total thyroidectomy has three rationales: (1) to destroy any residual microscopic foci of disease, (2) to increase specificity of subsequent 131 I scanning for detection of recurrent or metastatic disease by elimination of uptake by residual normal tissue and (3) to improve the value of measurements of serum Tg as a serum marker derived only from malignant thyroid cells. [69] Retrospective data from several studies suggest that radioiodine ablation reduces long-term disease-specific mortality in patients with primary tumors that are at least 1 cm in diameter, are multicentric or have soft tissue invasion at presentation. [34],[70],[71],[72] Ablation is generally not recommended for solitary primary tumors < 1 cm unless there is evidence of extrathyroidal invasion or metastasis. According to the American Thyroid Association guidelines, radioiodine is administered to all patients with stage III and stage IV disease. Ablation is recommended to all patients < 45 years and most patients over 45 years with stage II disease. For patients with stage I disease, ablation is recommended for those with tumors that are multifocal, show vascular invasion and aggressive histology. For maximum radioiodine uptake after thyroidectomy, concentrations of thyroid hormone should drop sufficiently to allow the endogenous thyroid stimulating hormone (TSH) concentration to rise above 25-30 mU/L. [73] Thyroxine has a half-life of 7 days and hence ablation is performed 4-8 weeks following surgery. When hypothyroidism is worrisome, triiodothyroinine can be supplemented instead of the more commonly used thyroxine, which can be used up to 2 weeks prior to ablation. [74] Other precautions include avoidance of iodine-rich foods for the 2 weeks prior to radioiodine administration as they interfere with its uptake. [75] The use of iodinated contrast for investigations suppresses thyroid iodine uptake for 1-3 months. [76] The utility of whole-body radioiodine scans using 37-185 mBq of 131 I prior to the administration of the ablative dose of radioiodine is debated. Its use identifies extra-thyroidal metastases, changing the treatment planning in terms of increasing the dose required to ablate the malignant load. However, the low doses of radioiodine used in the scans have been reported to reduce uptake of the subsequent ablative or treatment dose in a process known as stunning. [77] Substitution of 123 I instead may avoid such stunning without affecting the diagnostic accuracy. [78] However, in the low likelihood of metastatic disease, the usefulness of scanning before treatment is not clear; most consensus guidelines note that scanning before ablation is optional. [79],[45] Empirical doses for ablation following total thyroidectomy typically is in the range of 2,778-5,556 mBq. However, lower doses have also been used. [80],[81] The effectiveness of such empirical therapy is about 80% and is significantly lower when surgery is inadequate or remnant load is high. [82] It is in such instances that whole-body scans are useful in increasing the effectivity of radioiodine ablation through the use of dosimetry to calculate accurate dosage. [83] Dosimetry however requires several measurements of uptake of a tracer radioiodine dose into the residual tissue, and hence is resource and labor intensive, but higher likelihood of successful ablation could result from the accurate dosing generated from its use. [84] When substantial locoregional disease is detected or excessive thyroid remnants are identified by scanning, additional surgery before radioiodine administration should be strongly considered. A scan is commonly performed after ablation and such postablative scans have a greater sensitivity to detect metastases than the preablative scans, thus guiding future treatment planning. [84] Radioiodine scans after 6-12 months are helpful in predicting the 10-year relapse-free survival. If the first scan is negative, it predicts a 10-year relapse-free survival of 90%. If the second scan is negative, a 95% relapse-free survival can be expected. [85] However, consensus guidelines recommend such scanning only in patients in whom clinical and radiological investigations suggest recurrence. Following ablation, lifelong supplementation of thyroid hormone is essential to prevent hypothyroidism and to keep TSH levels to a minimum, preventing stimulation of remnant or dormant thyroid cells. [86] The level of TSH is to be maintained between 0·1 and 0·5 mU/L in patients with a low risk of thyroid cancer morbidity and mortality and below 0.01 mU/L in case of high-risk patients. [87] Suppression therapy has been associated with side-effects such as increased bone turnover, increased risk for supraventricular tachycardia and exacerbation of ischemic heart disease and hence should be used judiciously. [88] Guidelines however differ on the duration of suppressive therapy, varying from 3 to 10 years. [89],[25] Follow-Up Despite the low mortality rate associated with PTC, recurrence after initial treatment, primarily in the form of regional LN metastases, is a major concern, occurring in 9-30% of patients. [90],[91],[92] Serum Tg, recombinant human TSH-stimulated Tg (stimulated Tg), cervical HRUSG, whole-body radioiodine scan, FDG-PET and Tg mRNA are the various investigations used in follow-up. Serum Tg is produced exclusively by thyroid follicular cells and their presence in peripheral blood after total thyroidectomy and remnant RAI ablation suggests the presence of residual, recurrent or metastatic disease. [93] Sensitivity of serum Tg is increased with increase in TSH levels, but its specificity is decreased with incomplete surgery or ablation. Use of thyroxine at a suppressive dose decreases the sensitivity of serum Tg from 85-90% to 50%. [94],[95] Recombinant human TSH-stimulated Tg was introduced to avoid the hypothyroidism that could occur with thyroid hormone withdrawal in sensitive patients and, at the same time, increase the sensitivity of the serum Tg assay. [96],[97] The recommendation for obtaining TSH-stimulated Tg levels is based on the observation that approximately 20% of patients who are clinically free of disease with TSH-suppressed Tg < 1 ng/mL will have a serum Tg level> 2 ng/mL after rh-TSH stimulation or thyroid hormone withdrawal. [98] Recombinant human TSH is particularly beneficial in patients who are unable to produce endogenous TSH due to hypopituitarism and in those in whom thyroid hormone withdrawal is contraindicated due to comorbid disease. Cervical HRUSG is highly sensitive in the identification of cervical metastases, including local-regional metastatic disease as small as 2-3 mm. [99],[100],[101] Local-regional metastases occasionally are detected by HRUSG even when stimulated serum Tg levels remain undetectable. [102] Patients with cervical disease account for the majority of low-level elevations in stimulated Tg levels and, in these patients, cervical HRUSG is highly sensitive in the detection of recurrence. In fact, cervical disease may be detected by US even when TSH-stimulated Tg levels remain undetectable. [102] The combination of HRUSG and stimulated Tg is the most reliable method for detection of recurrent disease. [103] Consensus guidelines recommend the use of 6-12-monthly serum Tg level measurement and annual cervical HRUSG. For patients with a negative cervical HRUSG but an unstimulated Tg> 1 ng/mL, additional radiographic evaluation is recommended to look for disease recurrence and to serve as a baseline for more imaging studies. It is in this situation that 18FDG-PET may find significance in identifying recurrent and metastatic disease. The usefulness of whole-body radioiodine scans has decreased in significance since the introduction of cervical HRUSG and serum Tg assays and, at present, may be useful to identify distant metastasis when other imaging modalities fail. [104] A more recent advancement is the use of serum Tg mRNA, again produced by thyroid follicular cells but, unlike serum Tg, is not affected by the presence of anti-Tg antibodies that interfere with the serum Tg immunometric assay. [105],[106] Given the low sensitivity and negative predictive value, 82% and 43% respectively, reported in one study and even lower specificity demonstrated in another, this newer modality must still be considered experimental pending further evaluation. [107] Management of Locoregional Recurrence The most worrisome aspect in the management of PTC is recurrent or persistent disease, cervical nodal metastasis being the most troublesome. For persistent or recurrent disease following surgery, management of nodules> 1 cm, surgical resection is the most appropriate as RAI treatment is unlikely to destroy disease of this size. For lesions < 1 cm and those with a negative HRUSG and a rising titer of Tg, the so-called "Tg-positive scan-negative" disease, radioiodine treatment with 100-150 mCi is recommended. Over the recent years, 18 FDG PET scanning has been demonstrated to have an important role in detecting non-RAI avid disease that is manifest primarily by persistent serum Tg levels. [108],[109] Advances in PET and increased availability has further improved our armamentarium to diagnose persistent or recurrent disease. In most studies, FDG PET scan identifies a metastatic lesion in 75-80% of serum Tg-positive, scan-negative patients. Management of Distant Metastasis Distant metastases are present in only 3-5% of patients who have PTC at diagnosis. They can become evident in as many as 9-10% during the course of follow-up. [110] 18 FDG PET scanning has been shown to accurately identify the non-RAI-responsive metastatic lesions that are metabolically active, destined to more rapid growth and predictive of death from disease within a few years. Patients who have structurally progressive macroscopic metastatic disease that is not responsive to RAI should be referred for consideration of a clinical trial or other systemic therapy. In the follow-up of patients who have distant metastases, it is important to pay particular attention to lesions that are in areas where continued growth into surrounding structures would result in serious morbidity. These include lesions in the brain, spinal column, weight-bearing bones, upper mediastinum near the great vessels and in the tracheo-esophageal groove. Progressive growth in individual metastatic lesions can result in acute neurovascular compromise, such as spinal cord compression, nerve root compression, superior vena cava syndrome or an acute central nervous system event from brain metastases. Often, the acute symptoms respond to high-dose glucocorticoid therapy followed by surgical resection or external beam irradiation. Usually, these medical emergencies are most rapidly palliated with surgical resection of the offending metastatic lesion. Depending on the clinical situation, the overall rate of disease progression and other underlying medical conditions, urgent EBRT is also a reasonable palliative measure. Although resection or EBRT to these lesions in the setting of wide-spread distant metastases is not curative, appropriate treatment can avert serious neurovascular symptoms or prevent seriously morbid complications. Genetic Predisposition Research has identified a genetic basis for the PTC. Santoro et al. [111] demonstrated in sporadic PTC that the fusion of the C-terminal RET tyrosine kinase-encoding domain to the promoter and N-terminal portion of unrelated genes resulted in a chimeric oncogene that was constitutively active. More than 15 thyroid-specific RET (previously known as PTC) molecular fusion oncogenes have been identified till date, all of which differ according to the C-terminal region of the heterologous gene. The resultant activation of the RET intrinsic tyrosine kinase system is similar to the effect of RET mutations in the MEN2 endocrine syndromes. The prevalence of RET/PTC in the thyroid cancers of children is> 50%, and in youngsters in Kiev and Belarus who developed PTC following exposure to radiation from the Chernobyl accident, the prevalence of such rearrangements is 67-87%. [4] Subsequently, the BRAF mutation (T17699A) was identified and was found to be prevalent in 35-65% of the tumors. Their presence was independent of the RET translocations. A much less frequent chromosomal rearrangement associated with PTC involves the neurotrophic receptor tyrosine kinase, NTRK1 (also known as TRK and TRKA). The presence of BRAF mutation was found to be associated with aggressive forms of PTC, characterized by extrathyroidal invasion, LN metastases, advanced tumor stage and tumor recurrence, while RET/PTC translocations have not been correlated with such aggressive behavior. Similar RET/PTC translocations have not been found to be associated with follicular and anaplastic carcinomas. Research on targeted therapy may, in the future, add to the treatment possibilities. Future Perspectives in the Management of PTC The latter half of the 20th century saw progress in the systemic therapies for the management of metastatic and advanced PTC. The discovery of key etiologic oncogenic mutations in PTC led to a flurry of research on targeted therapy for advanced thyroid cancers. Somatic mutations in the signaling kinases BRAF and RAS, and the unique RET/PTC rearrangements seen in papillary carcinomas, led to constitutive activation of upstream signaling via the mitogen-activated protein kinase pathway. Various growth receptors like VEGF and EGFR also follow the kinase pathway. Evidence from transgenic animal models, as well as analysis of papillary microcarcinomas and radiation-induced chromosomal changes, all support the contention that most papillary carcinomas arise as a result of a single activating mutation in one of these three genes. [112] Some of the targeted kinase inhibitors are motesanib diphosphate, vandetanib, sorafenib, axitinib, imitinib, gefitinib, sunitinib and XL-184. Angiogenesis inhibitors, especially VEGFR inhibitors, have produced the most impressive clinical responses to date. [113] Further trials in the future might give the physician better options in the management of advanced and metastatic PTC where surgery is not feasible or unwarranted. Conclusion The PTC can be better diagnosed with FNAB, where a good number of procedures is performed every year. Cervical HRUSG has proven its efficiency in diagnosing the thyroid disease and LN metastases. With increasing numbers of cervical HRUSG being performed, the results are more or less reproducible. The controversy regarding the extent of thyroidectomy in patients of PTC is relatively settled. The LN metastasis does not seem to affect the overall survival, but it does increase the recurrence rate. It is worthwhile to offer LN dissection at initial surgery if LNs are ultrasonologically diagnosed to harbor malignancy. In experts hand, the rate of recurrent laryngeal nerve injury and hypoparathyroidism is negligible in a neck dissection in initial surgery but is likely to rise if surgery is performed for recurrent disease. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10049t1.jpg] [cn10049t2.jpg] |
| |||||||||

{kind=link}
{kind=link}