 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
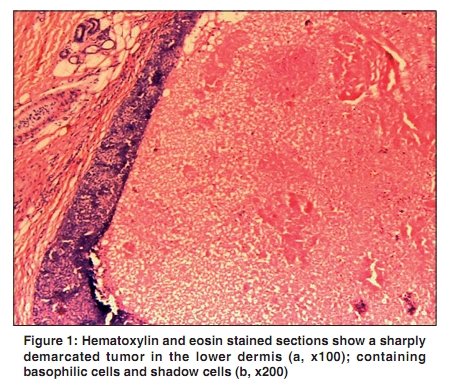
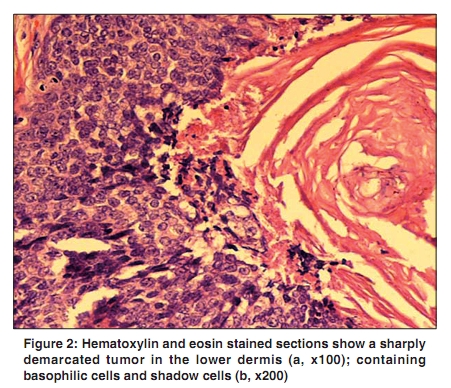
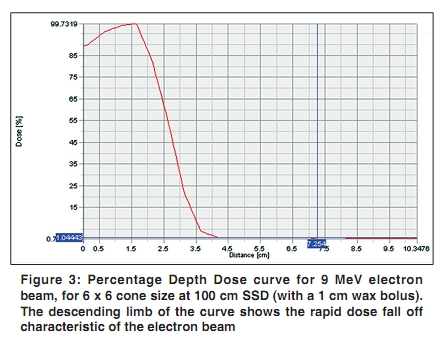
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 217-219 Letter To Editor Recurrent pilomatrix carcinoma of scalp treated by electron beam radiation therapy Bhasker S, Bajpai V1, Bahl A, Kalyanakuppam S Department of Radiotherapy, 1Biophysics, All India Institute of Medical Sciences, New Delhi, India Correspondence Address: Dr. Suman Bhasker, Department of Radiotherapy, All India Institute of Medical Sciences, New Delhi, India bhaskersuman@rediffmail.com Code Number: cn10050 PMID: 20448389 DOI: 10.4103/0019-509X.62995 Pilomatrix carcinoma is the malignant variant of Pilomatrixoma, a benign growth of the hair matrix cells. The benign form was described by Malherbe and Chenantais in 1880. [1] However it was only in 1980 that the malignant variant was first described by Lopansri and Mihm. [2] To date less than 80 cases of pilomatrix carcinoma have been reported from world over and the metastatic disease is even rarer, with only 12 cases of metastatic pilomatrix carcinoma having been reported. [3] This tumor occurs commonly in people in the middle to older age group. It commonly occurs in the head and neck region, although the upper extremity, trunk, and lower extremity are the other possible sites of involvement. A recurrence rate of 59% has been reported 5 - 17 months after surgical excision. [4] Metastasis to various sites including lung, liver, heart, and brain has also been described. Wide surgical excision is the mainstay of treatment for this tumor. [5] There is little clinical experience with the use of postoperative radiation therapy. Electron beam radiation, which offers a unique control in accordance with the depth of the tumor, may be especially suited for treatment of these tumors particularly in a recurrent setting. A 45-year-female was referred to our clinic with a history of developing recurrent swelling on her scalp 18 months back. She underwent a wide excision of the mass. Postoperative histopathology showed a circumscribed tumor with follicular differentiation, keratinization, and stromal foreign body giant cell reaction. There were areas of necrosis, nuclear atypia, and brisk mitosis. The features were suggestive of malignant pilomatrixoma. No adjuvant treatment was given to the patient. The tumor recurred after six months. On presentation to us the patient had an ulceroproliferative mass, 1.5 x 1.0 cm, over the right parietal scalp region. The growth was firm and nontender. There was no lymphadenopathy. A hemogram and biochemistry profile was normal. Chest X Ray evaluation was normal. The patient was diagnosed as having rT2N0M0 disease (Stage II). The patient again underwent wide local excision of the mass. Excised tissue submitted for histopathological examination was fixed in 10% buffered formalin, processed, and paraffin embedded. Five micron thick sections were cut and stained with Hematoxylin and Eosin. A microscopic examination revealed a sharply demarcated tumor in the lower dermis and subcutaneous fat. The tumor was composed of basophilic cells along the periphery of the tumor islands and shadow cells. Mitotic figures with a maximum of 9/10 per HPF (high power field) were seen. The resected margins were free. The histological features were diagnostic of pilomatrix carcinoma [Figure - 1] and [Figure - 2]. In view of the recurrent nature the patient was planned for postoperative radiation therapy to a dose of 50 Gray over 25 fractions. The patient was planned for electron beam radiation therapy. A radiation dose of 50 Gray over 20 fractions was delivered using a 9 MeV electron beam on Clinac 2300 CD linear accelerator, (Varian Medical System Inc. USA). For dosimetric evaluation EclipseTM treatment planning system (Varian Medical System Inc. USA) was used. A single radiation field of size 6 x 5 cm was planned for the affected scalp. A wax bolus of 1 cm was used to increase the dose to the skin. The patient tolerated the treatment well. Grade 2 skin reaction was observed during the course of radiotherapy and it was managed conservatively. At a one-year follow up the patient was disease-free. Recurrences are well-documented in pilomatrix carcinoma after initial surgical treatment. Radiation therapy can be used in an adjuvant setting, particularly in recurrent cases undergoing repeat surgical excision. Tselis et al. have shown both external beam and interstitial brachytherapy to be effective in the treatment of pilomatrix carcinoma. [6] Veliath et al. treated a case of pilomatrix carcinoma using radiation therapy alone to a dose of 45 Gy in three weeks. The patient was disease-free at a three-year follow up. [7] Radiation therapy is an acceptable alternative for the treatment of many malignancies of the skin. The results are gratifying, and long-term sequelae are few. In basal cell and squamous cell carcinomas, radiation is often the best treatment when surgery is expected to cause excessive morbidity or mortality or require extensive reconstruction. [8],[9],[10],[11],[12] Electron-beam therapy is a useful radiation modality to treat superficial skin tumors less than 5 cm deep. Various studies have shown that electron-beam treatment is not inferior to superficial x-ray treatment and even better for larger tumors. [13],[14] Electron-beam therapy has been extensively used to treat cutaneous tumors, with good functional and cosmetic results. [15],[16] Different electron energies of 6 Mev, 9 Mev, 12 Mev, 16 Mev, and 20 Mev are available for treatment purpose. The depth of treatment can be controlled by selecting the appropriate electron-beam energy, and the radiation dose rapidly falls to near zero in the normal tissues below the specified depth, thus reducing the dose to the underlying normal tissues with decreased radiation-associated toxicity. [17] Low-energy electron irradiation of the whole skin is used to treat skin diseases such as mycosis fungoides. [18],[19],[20],[21] In our patient the skin dose achieved was 88.5% (49.5 Gy) of the prescription dose. A 2-cm depth of the affected scalp region was treated to the prescription dose of 50 Gray. The dose at D max (The point of maximum dose on the central axis of the isodose curve) was 55.5 Gray. The radiation dose was negligible at a depth of 3.5 cm from the surface of the scalp [Figure - 3]. The mean dose received by the underlying brain tissue was only 1.7 Gray. Such a minimal dose can be easily tolerated by the brain tissue without any acute or long-term toxicity A decreased recurrence rate has been reported with the use of radiotherapy, postoperatively. [3],[22] Radiotherapy can also be practiced in patients in whom surgical excision is not possible. Electron-beam therapy is an effective modality for the management of superficial skin tumors. It can be effectively used in recurrent pilomatrix carcinoma to increase the local control rates. The role of chemotherapy remains undefined. Various chemotherapy agents such as Cisplatinum along with 5 Fluorouracil, or paclitaxel, have been tried to treat metastatic cases of pilomatrix carcinoma, without success. [23],[24],[25] References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10050f3.jpg] [cn10050f1.jpg] [cn10050f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}