 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
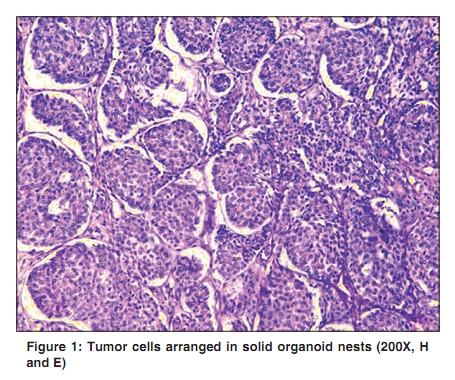
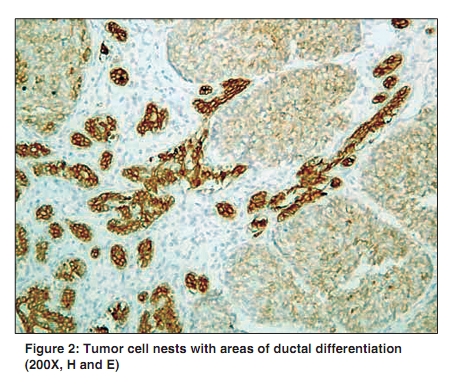
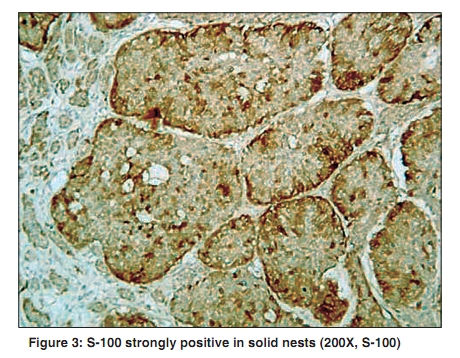
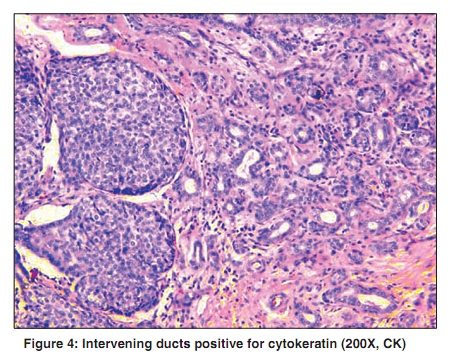
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 219-220 Letter To Editor Sialoblastoma: A rare salivary gland neoplasm Kattoor J, Baisakh MR, Mathew A, Somanathan T, Nayak N, Abraham EK Department of Pathology, Regional Cancer Center, Trivandrum- 11, Kerala, India Correspondence Address: Dr. Manas R Baisakh, Department of Pathology, Regional Cancer Center, Trivandrum- 11, Kerala, India drmbaisakh@gmail.com Code Number: cn10051 PMID: 20448390 DOI: 10.4103/0019-509X.62996 Sir, Salivary gland tumors account for 8% of all pediatric head and neck tumors. Less than 0.25% occurred in children younger than 10 years. [1],[2] Sialoblastoma is an extremely rare, potentially aggressive, salivary gland neoplasm that recapitulates the primitive salivary analage and usually presents at or shortly after birth. A one-year-old male child was brought to the hospital with a complaint of swelling over the right cheek, which was gradually increasing in size. The patient had a past history of swelling over the same cheek since birth, and had been operated upon two months earlier. No previous biopsy reports were available with the patient. On examination, there was a firm, nontender swelling over the parotid area. No cranial nerve deficit was demonstrated. Computer tomography (CT) showed a nonhomogenous mass adherent to the underlying bone. The biopsy showed a cellular neoplasm composed of monomorphic to pleomorphic basaloid tumor cells, arranged in lobules and nests [Figure - 1]. At places, few rosette-like structures were seen. The nucleoli were inconspicuous and the cells had a scanty cytoplasm. Mitosis was 2 - 3 / High power field (HPF). Eosinophilic fibrillar material was seen in the background. Few ducts lined by cuboidal epithelium were seen in between [Figure - 2]. Immunohistochemistry revealed tumor cells positive for S-100 [Figure - 3] and ducts positive for cytokeratin [Figure - 4]. Hence, a diagnosis of sialoblastoma was offered. Superficial parotidectomy with preservation of facial nerve had been done for the initial lesion. A radical approach was followed for the recurrent disease. A partial right maxillectomy, along with removal of residual parotid tissue and resection of the facial nerve was performed. A chemotherapy regimen comprising of vincristine, doxorubicin, and cyclophosphamide, alternating with cisplatin and etoposide for a total of four courses, was administered, followed by radiotherapy. The patient remained disease-free during one year of follow up. Salivary gland neoplasms in children are rare. These account for < 3% of the patients with primary salivary gland tumors, a majority of them between the age of 5 and 16 years. Vawter and Teft [3] in 1966, proposed the term ′embryoma′ for salivary gland tumors present since birth or noticed thereafter. The earliest sialoblastoma was reported at 37 weeks of gestation and diagnosed by intrauterine ultrasonography. [4] It is a locally aggressive tumor with a propensity to recur and can metastasize regionally Surgical excision is the primary treatment of choice. However, adjuvant chemotherapy and radiotherapy have been advocated for cases with local recurrence and regional metastatic disease. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10051f4.jpg] [cn10051f1.jpg] [cn10051f3.jpg] [cn10051f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}