 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
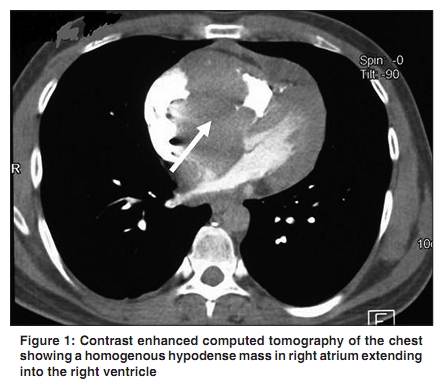
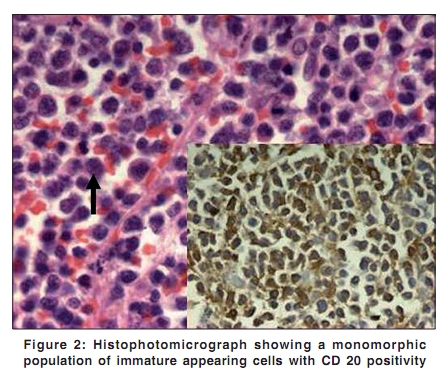
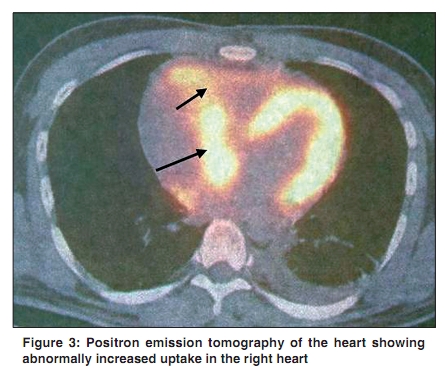
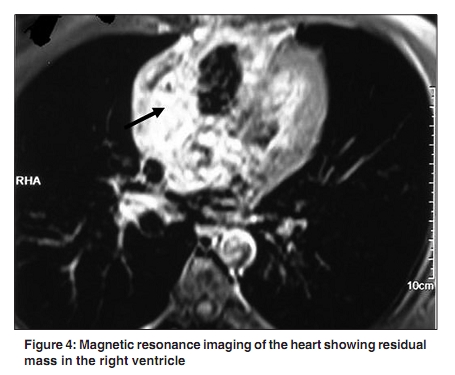
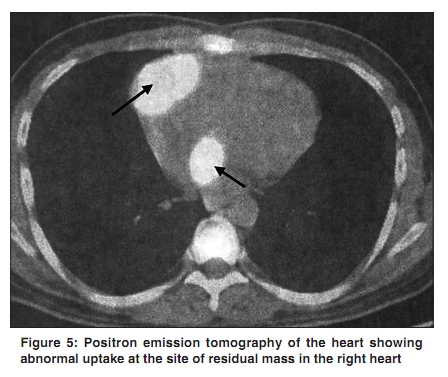
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 220-222 Letter To Editor Heart as the site of first relapse in diffuse large B-cell lymphoma Singhal M, Raina V, Medhi K, Gupta C1, Reddy RM2 Departments of Medical Oncology, 1 Pathology, 2 Nuclear Medicine, IRCH, All India Institute of Medical Sciences (AIIMS), New Delhi, India. Correspondence Address: Dr. Manish Singhal MD, Department of Medical Oncology, IRCH, All India Institute of Medical Sciences (AIIMS), New Delhi, India singhaloncocare@yahoo.co.in Code Number: cn10052 PMID: 20448391 DOI: 10.4103/0019-509X.62999 Sir, Metastatic involvement of the heart occurs most commonly from lung and breast cancer, and malignant melanoma. While primary lymphoma of the heart is well described, malignant lymphoma metastasizing to the heart, is much more common and is present in up to 20% of cases taken to autopsy. [1] However, an antemortem diagnosis of secondary involvement of heart by malignant lymphoma is not only difficult but rare. In a clinicopathologic study of 25 autopsy cases, all were secondary cardiac lymphoma, and none were diagnosed before death. [2] Extensive cardiac involvement with malignant lymphomatous disease can occur in patients with acquired immunodeficiency syndrome or as a direct extension from surrounding malignant lymphoid tissue. However, literature describing heart as a separate and single site of relapse in a case of lymphoma is scarce (one case report). [3] A 27-year-old healthy male, presented with left-sided lumbar pain of one month duration. He was found to have a left renal fossa mass measuring 14 Χ 9 cm, as the sole site of disease, biopsy of which showed large B-cell non-Hodgkins Lymphoma (NHL), positive for CD20 and CD45 and negative for CD99, neuron-specific enolase and cytokeratin. Baseline echocardiography had no evidence of intracardiac mass/lesion at that time. He received six cycles of CHOP (cyclophosphamide, doxorubicin, vincristine and prednisolone), following which there was a residual mass of 5 Χ 3.6 cm. Positron emission tomography (PET) showed no significant fluorodeoxyglucose (FDG) uptake suggesting an inactive lesion and he was advised close follow-up. Three months later, he presented with complaint of dyspnea and palpitations of 15 days duration. Echocardiography revealed a large mass in the right atrium. Contrast enhanced computed tomography (CECT) of the chest showed a 8.5 Χ 7 cm homogenous hypodense mass in right atrium extending into right ventricle [Figure - 1], indenting right ventricle outflow tract. Interatrial septum was infiltrated with extracardiac and left atrial extension. There was no mediastinal or hilar lymphadenopathy. Necrosis and calcification was evident in the primary lesion in left paranephric space. Patient was taken for an urgent open cardiac surgery and right atrial mass was excised. Histopathological examination of the mass was compatible with NHL - B cell immunophenotype [Figure - 2]. Patient was seronegative for human immunodeficiency virus (HIV). Postoperative PET scanning showed increased uptake in the heart suggesting residual tumor [Figure - 3]. He was started on chemotherapy with rituximab and DHAP regimen (dexamethasone, cisplatin and cytarabine) on day 14 post-op. After three cycles of chemotherapy, Magnetic Resonance Imaging (MRI) of the heart and PET showed residual mass in the right ventricle [Figure - 4] and [Figure - 5] along with new lesions appearing in right renal area suggesting progressive disease. Patient was taken up for high-dose chemotherapy - autologous stem cell transplantation (HDCT - ASCT) as a desperate measure. Unfortunately, he expired on day 10 of ASCT as a result of severe sepsis and cardiac failure. Lymphoma relapsing in the heart in a healthy, HIV seronegative host is a marker of aggressive disease and confers poor prognosis, making early and timely diagnosis important. [3] Modern techniques such as transesophageal echocardiography (TEE) including TEE-guided transvenous biopsy and non-invasive modalities such as PET may prove useful tools in this regard. [4],[5] While clinicians must keep note of this unique possibility for its early and timely diagnosis; lymphoma relapsing in the heart needs aggressive anti-lymphoma therapy, which may be followed by HDCT - ASCT as a consolidative measure for these high risk patients. [6] References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10052f5.jpg] [cn10052f2.jpg] [cn10052f3.jpg] [cn10052f1.jpg] [cn10052f4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}