 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
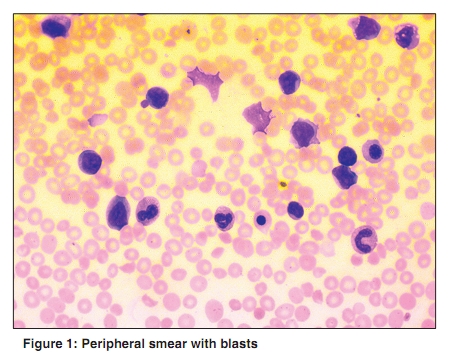
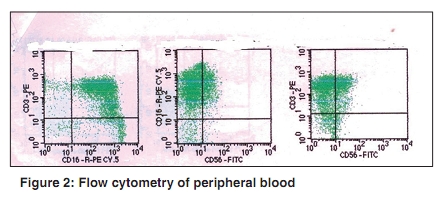
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 222-223 Letter To Editor Lymphoma masquerading as acute leukemia-mystery unfolded Jain P, Prabhash K, Menon H, Gupta S, Parikh PM Department of Medical Oncology, Tata Memorial Hospital, Dr. E. Borges Road, Parel, Mumbai, India Correspondence Address: Dr. Preetesh Jain, Department of Medical Oncology, Tata Memorial Hospital, Dr. E. Borges Road, Parel, Mumbai, India pjain@nshs.edu Code Number: cn10053 PMID: 20448392 DOI: 10.4103/0019-509X.63001 Sir, Two young adult male patients who presented with signs and symptoms similar to acute leukemia are discussed in this report. Patient A was pretreated outside with five cycles of standard cyclophosphamide, doxorubicin, vincristine, and prednisone (CHOP) chemotherapy six months back and underwent splenectomy before presenting to us. He had pallor, icterus, hepatomegaly (20 cm), generalized lymphadenopathy, ascites and anemia, thrombocytopenia, total leucocyte count of 90,000 Χ 109 cells with 56% blasts [Figure - 1], and impaired liver and renal function tests. On evaluation, marrow aspirate immunophenotyping was negative for B- and these T-cell markers (CD4, CD8, CD5, TCRαβ) and positive for CD3, CD7, CD16, CD56 (Dim), and TCRγδ [Figure - 2]. Postsplenctomy histopathology showed sinusoidal infiltration by CD3 positive T cells. Fluorescence in situ hybridization (FISH) analysis of marrow was positive for iso7q. Patient B presented with fever and epistaxis and had severe pallor, subconjuctival hemorrhage and hepatosplenomegaly (17 and 6 cm). The peripheral smear had 78% blasts and total leucocyte count of 56000 Χ 109 cells with platelet count of 20,000 Χ 109 cells. Marrow aspirate showed hypercellular marrow with 86% blasts. Marrow immunophenotype was positive for CD2, CD3, CD7, CD8, CD16, CD56, cyto CD3, and TCRγδ and negative for CD4, TCRαβ, CD5, and B-cell and myeloid markers. FISH analysis was negative for any numerical or structural aberrations in chromosomes 1, 7, 11, and 14. Both patients were treated with modified BFM 90 induction; patient A could tolerate treatment for four weeks but succumbed to neutropenic sepsis. Patient B is in complete remission and is on maintenance chemotherapy. Present case signifies the clinical importance of carefully planned immunophenotyping and its impact on timely treatment. Hepatosplenic T-cell lymphoma (HSTCL) is a rare entity that represents a very small portion of adult mature T-cell neoplasms. It is characterized by an aggressive clinical course and unfavorable prognosis. [1],[2] HSTCL predominantly affects young males and presents with B symptoms, pancytopenia, hepatosplenomegaly, and absence of nodal enlargement. A typical splenic, hepatic, and bone marrow sinusoid infiltration is present. Pathological cells of T-cell origin are characterized by a specific profile: CD2, CD3, CD7, γδ TCR positivity and CD5 and CD8 negativity. The TCR gamma-delta gene is always clonally rearranged, TIA-1 is almost always present, but commonly granzyme B and perforin are not present, indicating a nonactivated cytotoxic T-cell phenotype. The primary recurrent chromosome abnormality in HSTCL is isochromosome 7q, although not all series have documented i(7q) abnormalities in HSTCL. Case series of HSTCL have been published. [3],[4] In one series of 45 patients, bone marrow involvement, lymphoma cells in blood, and leucocytopenia were noted in 26 / 36 (72%), 16 / 32(50%), and 15 / 33 (45%) of the patients. HSTCL commonly involves the bone marrow, and different patterns of involvement have been reported, including exclusively sinusoidal, interstitial, and mixed sinusoidal and interstitial. Although marrow involvement and lymphoma cells in blood are frequent occurrences in HSTCL, leukemia-like presentation, as in the cases described above is uncommon [5] and standard treatment is not known, but intensive chemotherapy may perhaps benefit the patients. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10053f1.jpg] [cn10053f2.jpg] |
| |||||||||

{kind=link}
{kind=link}