 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
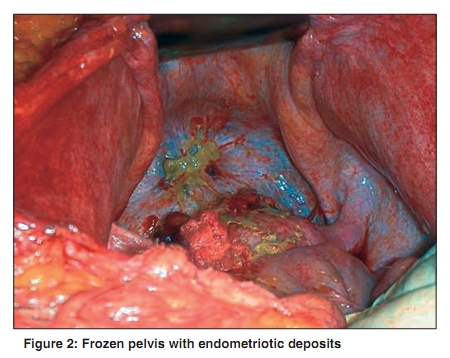
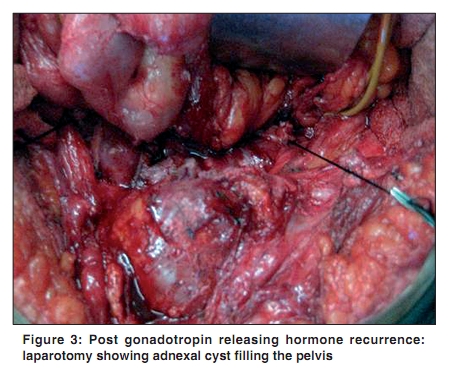
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 224-225 Letter To Editor Endometriosis with massive hemorrhagic ascites Suchetha S, Rema P, Mathew AP, Sebastian P Division of Surgical Oncology, Regional Cancer Centre,Thiruvananthapuram, India Correspondence Address: Dr. Sambasivan Suchetha, Division of Surgical Oncology, Regional Cancer Centre,Thiruvananthapuram, India suchethajyothish@gmail.com Code Number: cn10054 PMID: 20448393 DOI: 10.4103/0019-509X.63004 Sir, A 36-year-old parous lady presented with massive ascites of 8 months duration. Pelvic examination revealed nodularity in the pouch of Douglas. Sonography and an abdominal computed tomography scan showed marked ascites and small nodular deposits over the uterus and pelvic peritoneum. Her CA 125 was elevated (>5,000 U). Paracentesis and cytological examination showed no malignant cells. Hence, diagnostic laparotomy was decided upon to rule out ovarian malignancy. At laparotomy, 6 L of coffee-colored ascitic fluid was drained out. The small bowel loops, omentum, transverse colon and stomach matted together forming an abdominal cocoon [Figure - 1]. The sigmoid colon was found densely adherent to the posterior surface of the uterus and both adnexae [Figure - 2]. Multiple fleshy deposits were seen over the left adnexa, bladder peritoneum, omentum and stomach. Multiple biopsies were taken from the deposits. The histopathologic report was endometriosis. She was given gonadotropin releasing hormone (GnRH) analogue leuprolide for 1 year and responded well. Three months later, the patient presented with bilateral ovarian masses with moderate hydronephrosis. Radiological evaluation showed cysts with solid areas inside. A laparotomy was planned to rule out malignancy. We could complete the surgery in spite of dense adhesions to the rectosigmoid and ileocaecal junction [Figure - 3]. Omentectomy was also performed, which showed pathological evidence of endometriotic deposits. Endometriosis with ascites is very rare and it presents a diagnostic dilemma for the clinician. Only sporadic cases have been reported. The pathogenesis of ascites associated with endometriosis remains speculative. Bernstein et al. suggested that the blood and endometrial cells that are shed into the peritoneal cavity might irritate and stimulate the peritoneum, resulting in ascites. [1],[2] Another contributing factor may be the obstruction of lymphatics in the diaphragm by extensive peritoneal endometriosis. [4] Free blood in the peritoneal cavity may act as an irritant, causing dense adhesion of the intraperitoneal structures, forming an abdominal cocoon. [3] Susceptibility to association of advanced endometriosis and genetic polymorphism has been studied among the Korean population, which suggested that the aryl hydrocarbon receptor repressor, GSTMM1 and glutathione-S-transferase T1 are associated with advanced-stage endometriosis. [5] In most of these cases, a diagnostic laparotomy and histopathologic confirmation of the diagnosis is required. Definitive management involves surgical removal of endometriosis tissues followed by long-term hormonal suppression therapy. Surgery may involve cystectomy or hysterectomy with salpingoophorectomy. Medical management described is progestational agents (depot provera, norethinodrel, norethindrone acetate), danazol and GnRH analogue. In inoperable patients, options include prolonged medical therapy following laparotomy and biopsy. Some authors have reported radiation menopause in such situations. Patients who undergo conservative surgery or medical management need close follow-up after stopping medical treatment because recurrence can occur when the hormonal suppression is withdrawn. There is a rare chance for developing malignancy as endometriod or clear cell carcinoma, especially in atypical endometriosis. The reported frequency of malignant transformation is 5-10%. [6] References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10054f3.jpg] [cn10054f1.jpg] [cn10054f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}