 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
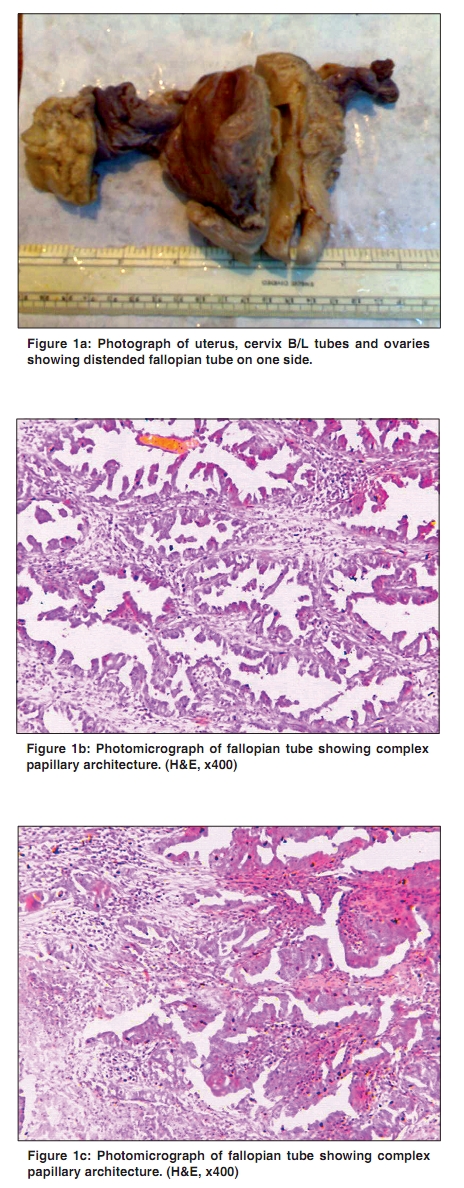
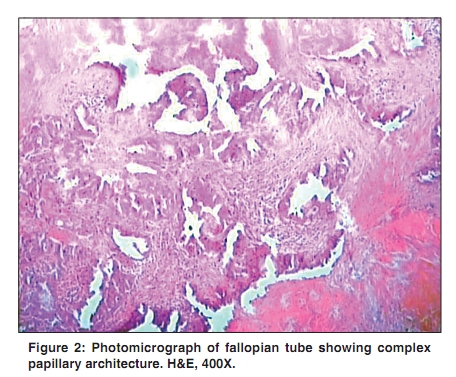
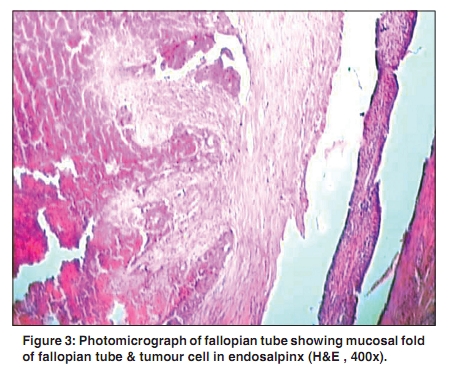
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 226-228 Letter To Editor Primary adenocarcinoma of fallopian tube Asotra S Department of Pathology, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India Correspondence Address: Ms. Sarita Asotra, Department of Pathology, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India saritaasotra@gmail.com Code Number: cn10056 PMID: 20448395 DOI: 10.4103/0019-509X.63008 Sir, Primary fallopian tube carcinoma is a very rare malignancy accounting for only 12% of all gynecologic cancers. We report a case of primary fallopian tube cancer in a 48-years-old female. Although fallopian tubes are frequently involved in benign gynecological conditions and are a common site for metastases, their primary malignant involvement is rare. [1] Because of its low prevalence, fallopian tube carcinoma is rarely diagnosed before surgery. [2] About 1500 to 2000 cases of fallopian tube cancer have been recorded worldwide. [3] It is more common for cancer to spread or metastasize, from other parts of the body, such as ovaries or endometrium than for cancer to actually originate in the fallopian tube. A 48-year-old lady was admitted with pain and ill-defined tender mass in the lower abdomen of the size 4.5 cm Χ 3.5 Χ 1 cm. Ultrasound examination showed a pelvic mass of possible ovarian origin arising from the right side. Total abdominal hysterectomy with bilateral salpingo-oophorectomy was done. Left side fallopian tube and both ovaries were grossly unremarkable. Other side fallopian tube measure 7 cm in length showing growth measuring 4.5 Χ 3.5 Χ 1 cm [Figure - 1]. C/S shows solid gray-white area with necrosis and papillae. M/E-Endometrium, myometrium, cervix, one side fallopian tube and both side ovaries unremarkable. Other fallopian tube growth shows highly pleomorphic cells arranged in fine branching papillae, acini and solid pattern. The nuclei are vesicular to hyperchromatic with conspicuous nucleoli at places and increased number of atypical mitotic figures. The tumor is invading into tubal muscularis layer [Figure - 2] and [Figure - 3]. Histological features are consistent with primary serous adenocarcinoma fallopian tube. Stage-1A. The endometrium, myometrium, cervix, both side ovaries and other side fallopian tube are free from tumor invasion. Primary fallopian tube carcinoma (PFTC) is a rare tumor that histologically and clinically resembles epithelial ovarian cancer (EOC).The diagnosis of PFTC is rarely considered preoperatively and is usually first appreciated by the pathologist. Primary fallopian tube carcinoma frequently occurs between fourth and sixth decade of life. The clinical sign and symptoms of PFTC are nonspecific, consisting of intermittent vaginal discharge, colicky pain relieved by discharge and abdominal mass and peri- or post-menopausal bleeding P/V in 50% of patients. Since it is difficult to differentiate PFTC from EOC, patients with at least one of the following criteria should have the diagnosis of PFTC. [4]
The International Federation of Gynecology and Obstetrics FIGO staging system assigns nearly two-thirds of patients to stage I or II and is based on surgical staging criteria similar to ovarian cancer. Primary adenocarcinoma of the fallopian tube with papillary features is most common histological type forming more than 90% of malignant tumor. The most important prognostic factor in fallopian tube carcinoma is stage of disease at laparotomy. In conclusion, fallopian tube cancer is a rare type of genital cancer, which is difficult to diagnose early and carries a poor prognosis. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10056f2.jpg] [cn10056f3.jpg] [cn10056f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}