 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
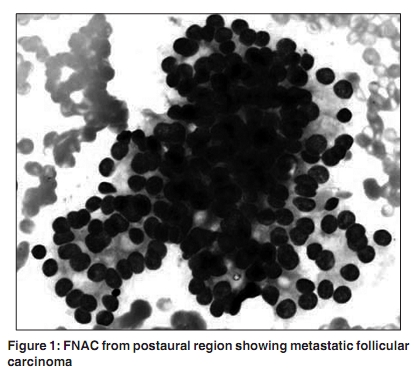
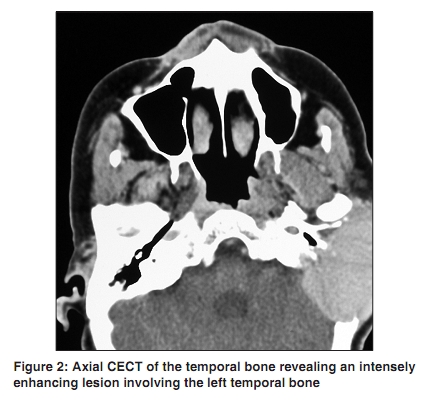
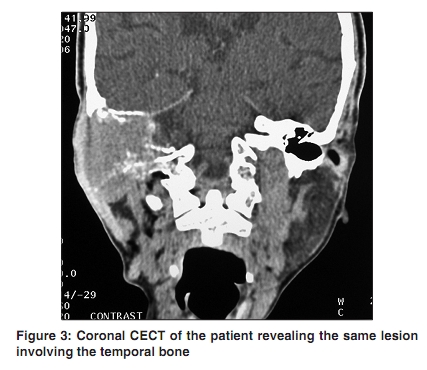
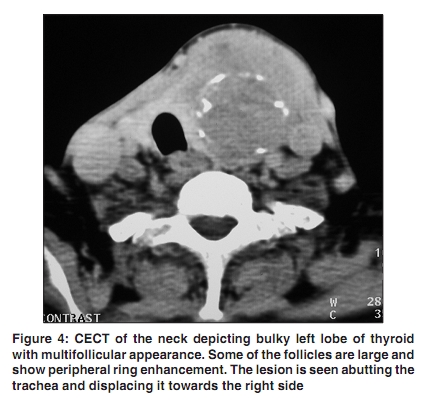
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 228-229 Letter To Editor Temporal bone metastasis from thyroid Raj A, Sayal A, Meher R, Girhotra M, Jain S1 Department of ENT and Head, Neck Surgery, and 1Pathology, MAM College and Assoc., LN Hospital, New Delhi, India Correspondence Address: Dr. Ankush Sayal, Department of ENT and Head, Neck Surgery, MAM College and Assoc., LN Hospital, New Delhi, India ankushsayal@yahoo.com Code Number: cn10057 PMID: 20448396 DOI: 10.4103/0019-509X.63012 Sir, Carcinoma metastasizing to the temporal bone is a rare entity. Most common secondary metastasis occurs from the breast (21.3%) followed by lung (12.8%), prostate (10.5%), skin (8.5%), cervix (6.4%), liver (6.4%), brain (4.3%), and oral cavity (2.1%). [1] Thyroid carcinoma metastasizing to the temporal bone is still rare. Very few case reports of thyroid carcinoma metastasizing to the temporal bone have been reported in the past. Review of literature reveals that in most case reports, the histological types have not been mentioned. [2] We describe here a case of a 60-year-old female, who presented with complaints of decreased hearing in the left ear, tinnitus for three months, recurrent multiple episodes of bleeding from the left ear, deviation of face for the past 13 days, and earache for 10 days, but no history of any ear discharge, vertigo, vomiting, seizures or loss of consciousness. Examination of the left ear revealed a diffuse, nontender, postaural swelling, a fleshy polypoidal mass in the external auditory canal and left Lower Motor Neuron facial palsy. Systemic examination revealed a 5 Χ 6 cm, hard, globular, neck swelling that moved with deglutition. According to the patient, this painless swelling had been there for the past 25 years, although she had noticed an increase in size during the past four months. Investigations (pure tone audiometry) revealed a conductive type of hearing loss and a polyp arising from the middle ear cavity on aural examination, under a microscope. Biopsy of the polypoidal mass and fine needle aspiration cytology (FNAC) from the postaural region revealed metastatic follicular carcinoma [Figure - 1]. On Contrast Enhanced Computed Tomography (CECT) of the temporal bone and neck, an intensely and homogenously enhancing lesion involving the left temporal bone with intracranial extension was noted [Figure - 2] and [Figure - 3]. The left lobe of the thyroid was found to be bulky, with a multifollicular appearance, without infiltration of the surrounding structures [Figure - 4]. Chest X-ray, ultrasound of the abdomen, and whole body scan did not reveal distant metastasis. The patient refused to undergo any surgical intervention and was therefore referred for radiotherapy. The most common site for involvement in metastasis to temporal bone is the petrous apex, probably owing to the sluggish blood supply at the petrous apex, followed by the tegmen tympani. [3],[4] Patients with temporal bone metastasis may remain asymptomatic or present with a variety of complaints, such as, sudden hearing loss, dizziness, tinnitus, facial palsy, otalgia, swelling behind the ear, bleeding from the ear, and even features of increased intracranial tension. Any patient presenting with facial palsy, sudden sensory neural hearing loss, and periauricular swelling should raise suspicion of a metastatic temporal bone tumor. [5] Such patients should undergo a detailed neurotological examination, pure tone audiometry, Brainstem Evoked Response Audiometry, and CECT of the temporal bone, brain, and the region of the primary. [6] Histological diagnosis should be established by a biopsy, FNAC or immunohistochemical analysis of the surgical specimen. Treatment for such cases usually consists of total thyroidectomy for the primary tumor and additional radioactive iodine therapy for any remaining metastatic thyroid tissue that is able to take up iodine. Caution should be exercised if imaging studies show metastatic thyroid tissue in the brain, because radioactive iodine therapy may cause tissue necrosis and brain swelling with intracranial hypertension and possible death. [7],[8] This case report adds to the growing list of rare yet possible metastasis to the temporal bone from a distant primary, and highlights the need for alertness of the treating physician when dealing with such cases. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10057f3.jpg] [cn10057f2.jpg] [cn10057f4.jpg] [cn10057f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}