 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
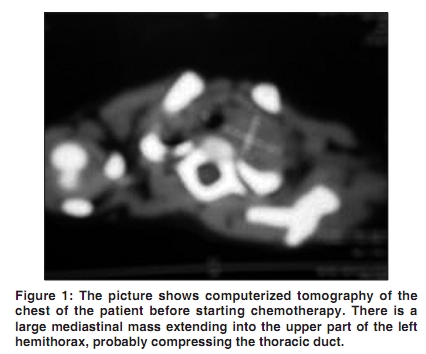
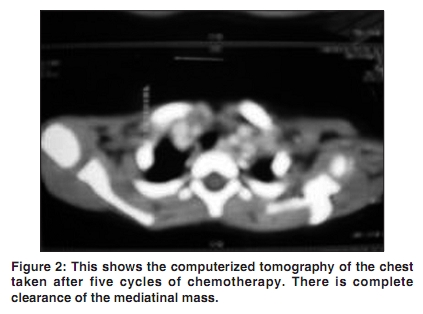
Indian Journal of Cancer, Vol. 47, No. 2, April-June, 2010, pp. 229-231 Letter To Editor Nontraumatic chylothorax in a case of neuroblastoma Seshachalam Arun, Nandennavar Manjunath, Laxmi LS, Sagar TG Department of Medical Oncology, Cancer Institute, Adyar, Chennai, India Correspondence Address: Dr Manjunath Nandennavar, Department of Medical Oncology, Cancer Institute, Adyar, Chennai, India min77@rediffmail.com Code Number: cn10058 PMID: 20448397 DOI: 10.4103/0019-509X.63014 Sir, A 2-year-old child presented with right eye proptosis and abdominal pain of 1 week duration. Examination showed left upper abdominal mass, right-sided proptosis and decreased air entry in the left side. Bone marrow biopsy showed small round malignant cells arranged in rosettes. Immunohistochemistry was positive for synaptophysin, chromogranin and neuron-specific enolase. The 24-h Vanillyl Mandelic Acid was elevated (75 mcg/dl). Computerized tomography (CT) scan of the abdomen revealed a large retroperitoneal mass arising from the left adrenal gland. CT scan of the chest showed a left paratracheal mass with right-sided pleural effusion [Figure - 1]. Magnetic resonance imaging of the brain revealed a hemorrhagic lesion in the frontoparietal region. Cerebrospinal fluid analysis was normal. MIBG scan showed multiple skull uptakes. The above investigations were suggestive of high-risk stage 4 neuroblastoma and the patient was started on CCG 3891 protocol treatment. On D15 of the first cycle of chemotherapy, he developed tachypnea and the chest X-ray revealed right-sided pleural effusion. Milky white fluid was obtained by diagnostic tapping and was sent for analysis. Electrophoretic analysis of the aspirated fluid showed a chylomicron band, cytology of the fluid showed lymphocytosis without any atypical cells and chemical analysis revealed a pleural fluid triglyceride level of 220 mg/dl and cholesterol of 50 mg/dl. All these investigations were conclusive of chylothorax. Intercostal tube drainage had to be performed to relieve the respiratory distress. The amount of fluid from the drain gradually reduced from 600 ml/day to 300 ml/day, and remained static for the next 2 weeks. A second cycle of CCG 3891 protocol with prophylactic growth factor had to be initiated to relieve the compressive effect of the left paratracheal mass on the chylous duct. Parenteral nutrition with 10% dextrose, 20% intralipid and aminoacid was initiated. He was also kept on a high-protein, low-fat and medium-chain triglyceride-containing diet. Fresh frozen plasma was transfused on alternate days. Despite 2 weeks of the above management, chyle drainage was persistent, which prompted us to start octreotide infusion. It was started at 0.5 μg/kg/h and was later escalated to 1.0 μg/kg/h. Chyle drainage slowly decreased and stopped completely after 4 days of starting octreotide infusion. Octreotide infusion was tapered over the next 2 days and then stopped. Intercostal tube drainage was removed after 3 weeks. Presently, the patient has completed five cycles of chemotherapy and has gained adequate weight, with no evidence of reaccumulation of chyle [Figure - 2]. Local treatment in the form of resection of abdominal mass is contemplated now, which will be followed by autologous transplantation and maintenance with cis retinoic acid for 1 year. Chylothorax is a life-threatening form of pleural effusion in childhood. [1] Its etiology may be either a congenital abnormality of the thoracic duct or traumatic (postoperative and surgical) and nontraumatic causes. Nontraumatic causes of chylothorax include neoplasm, aneurysm, inflammatory disease and subclavian thrombosis. [2] Because chyle is rich in protein and lymphocytes, large losses result in malnutrition and immune suppression. This mandates nutritional support either by parenteral hyperalimentation or medium-chain triglyceride-rich diet. [1] Most of the cases of chylothorax are managed with pleural drainage, use of medium-chain triglyceride oils, fat-free alimentation or enteric rest. Surgical management is indicated when the chyle drainage is persistent despite conservative measures. [3],[4] Somatostatin and octreotide (a somatostatin analogue) has been reported to reduce chyle production by decreasing splanchnic circulation. [5] In our case, octreotide infusion led to stoppage of chyle accumulation in the pleural space and no adverse effects were documented. References
Copyright 2010 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn10058f2.jpg] [cn10058f1.jpg] |
| |||||||||

{kind=link}
{kind=link}