 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
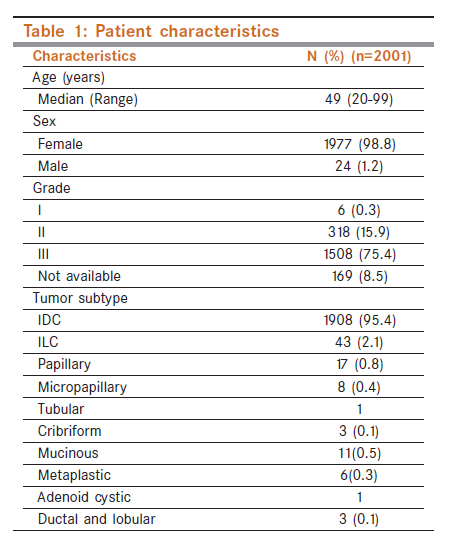
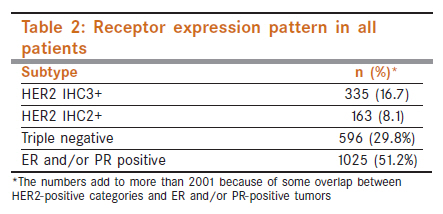
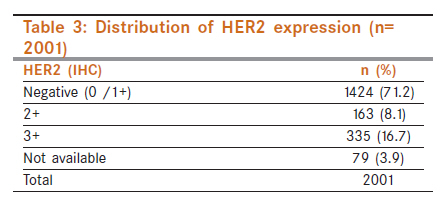
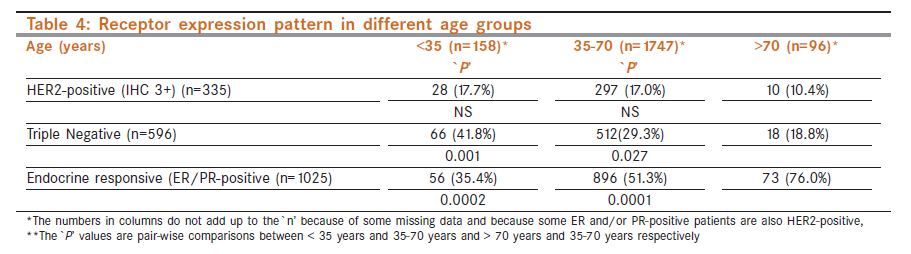
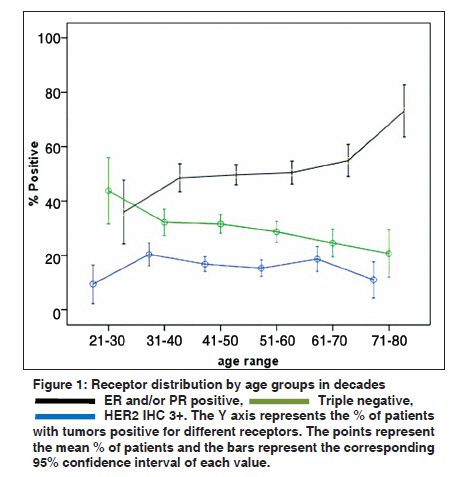
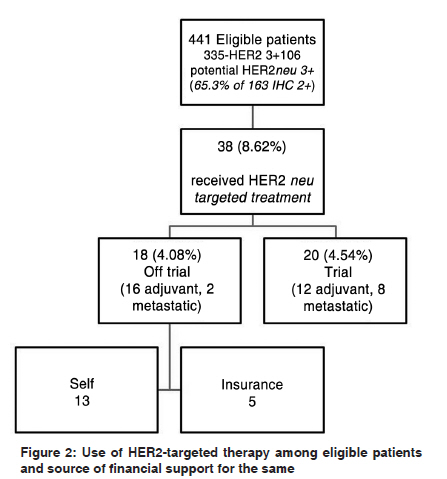
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 391-396 Breast - Original Article Estrogen, progesterone and HER2 receptor expression in breast tumors of patients, and their usage of HER2-targeted therapy, in a tertiary care centre in India J Ghosh1, S Gupta1, S Desai2, T Shet2, S Radhakrishnan1, P Suryavanshi2, V Parmar3, R Jalali4, G Goyal1, R Hawaldar5, A Patil2, N Nair3, RA Badwe3 1 Department of Medical Oncology, Tata Memorial Centre, Mumbai, Maharashtra, India Code Number: cn11114 PMID: 22293249 Abstract Background: This study was undertaken to document the pattern of expression of estrogen (ER), progesterone (PR) and human epidermal growth factor receptor-2 (HER2) and the usage of HER2-targeted therapy in a large tertiary care hospital in India in the year 2008.Materials and Methods: The histopathology reports of all breast cancer patients registered in the hospital in 2008 were extracted from the electronic medical record system. All the cases were immunohistochemically evaluated for estrogen and progesterone receptor status (ER and PR), and c-erbB-2 protein (HER2) expression using standard immunoperoxidase method. The use of HER2-targeted therapies was evaluated by extracting relevant information from the database of the hospital pharmacy and case charts of patients enrolled in ongoing approved trials. Results: A total of 2001 new patients of invasive breast cancers with available pathology reports were registered in the hospital in the year 2008. ER and/or PR expression was positive in tumors of 1025 (51.2%) patients. HER2 3+ expression by immunohistochemistry (IHC) was found in 335 (16.7%) and HER2 2+ in 163 (8.1%). The triple negative phenotype was found in 596 (29.8%) patients. An estimated 441 patients were eligible to receive HER2-targeted therapy based on their HER2 status. Of these 38 (8.6%) patients received some form of HER2-targeted therapy; 20 patients (4.5%) as part of ongoing clinical trials and 18 (4.1%) as part of routine care. Conclusions: The overwhelming majority of patients eligible for HER2-targeted therapy in our institution are unable to receive it because of financial constraints and limited access to health insurance. There is a higher fraction of patients with the triple negative phenotype compared to the Western population. Keywords: HER2-targeted therapy, India, triple negative Introduction Breast cancer is the most common cancer among women in the urban Indian population and second only to cancer of the cervix in the rural population, based on cancer registry data. [1] The data regarding the proportion of breast cancer patients from India who are human epidermal growth factor receptor-2 (HER2)-positive is sparse. Approximately 25-30% of all breast cancers have been reported to over-express HER2 in the Western literature. [2] A number of studies have established that HER2 over-expression is a poor prognostic factor in patients with early breast cancer. [3] The development of trastuzumab, a humanized monoclonal antibody against the extracellular domain of HER2 and other targeted therapies has led to a marked improvement in the outcome of patients with early and metastatic breast cancer whose tumors over-express the HER2 receptor. [4],[5] However, trastuzumab is an expensive treatment that is beyond the reach of the majority of patients in developing countries, who have thus not benefited from this advance. We undertook this retrospective study to quantify the proportion of HER2-positive patients who receive HER2-targeted therapy in a large tertiary cancer centre that draws patients from many parts of India. A secondary aim was to ascertain the receptor expression profile of newly diagnosed breast cancer patients in our institution in one calendar year. Materials and Methods This is a retrospective analysis that was conducted in the cohort of breast cancer patients who first presented to our tertiary care hospital, in the year 2008. The eligibility criteria included a histopathologically proven diagnosis of invasive breast cancer, with a pathology review available from our institution. The histopathology reports were accessed from the Hospital Electronic Medical Records System. Any ambiguity in the report was resolved through discussion with the pathologists. The clinical data were collected from the patient case charts that were available with the Medical Records Department. Information was collected on age, sex, Scarf Bloom Richardson grade, estrogen (ER), progesterone (PR) and HER2 receptor status by immunohistochemistry (IHC) and fluorescent in situ hybridization (FISH), usage of HER2-targeted therapy, enrolment in a clinical trial of HER2-targeted treatment, and health insurance status. The information on the usage of drugs was collated by accessing the electronic database of the Hospital Pharmacy and cross-checked and supplemented from the patient records. This was entered in a previously designed case record form and analyzed in SPSS Version 14.0. Methodology for immunohistochemistry All the cases were immunohistochemically evaluated for estrogen and progesterone hormone receptor status, (ER and PR) and c-erbB-2 protein (HER2) expression using standard immunoperoxidase method i.e. avidin-biotin complex peroxidase method (Vector peroxidase ABC kit - PK4001 and PK4002) and pressure cooking for antigen retrieval. Adequate tissue fixation in 10% neutral buffered formalin for 6-48 h was ensured. Paraffin sections (3-4 μm thick) with maximum invasive tumor component were selected for IHC. The antibodies used for ER, PR and c-erbB2 were monoclonal mouse anti-Human Estrogen Receptor, DAKO (Clone 1D5; dilution 1:50), monoclonal mouse anti-Human Progesterone Receptor, DAKO (Clone PgR 636; dilution 1:50) and 3B5 monoclonal antibody (Immunotech, dilution 1:10) respectively. The scores for ER and PR were calculated using the Shousha method. [6] On low power, the area of tumor cells showing nuclear positivity was graded as 1, 2 or 3 depending on the percentage of positive cells (< 1/3rds, < 2/3rds or > 2/3rds respectively). Likewise, the intensity of the nuclear staining was graded as mild (Score 1), moderate (Score 2) or intense (Score 3). Multiplication of these two scores (area x intensity) gives the score for the ER and PR status. Thus the maximum possible score was 9. A minimum score of 1 was required to categorize a tumor as positive for ER or PR. All the tests were interpreted with negative and positive controls. Staining of the nuclei of the normal ductal epithelium was used as the internal control for ER and PR staining while interpreting the slides. HER2 scoring of IHC slides was done as per the recommended American Society of Clinical Oncology ASCO guidelines 2007. Score 0 and Score 1 were considered as negative while Score 2 and Score 3 were considered as equivocal and positive respectively. Sections which showed strong membrane staining of normal epithelia of the breast were rejected and subjected to a repeat IHC. ER and PR scoring was done by assigning a score from 1 to 9 based on percentage distribution of immunoreactive tumor cells and intensity of staining. Cases in which internal control was negative were repeated. All the tests were interpreted in conjunction with positive and negative controls and if required, were repeated. Methodology for fluorescent in situ hybridization FISH was performed using the United States Food and Drug Administration (US FDA ) approved PathVysion (Abbott Molecular) HER2 DNA Probe kit, a dual-colored probe comprising locus specific identifier (LSI) HER2/neu SpectrumOrange and centromere enumeration probe (CEP) 17 SpectrumGreen. The test was carried out on paraffin sections obtained on acid-treated double poly-L-lysine-coated glass slides. The FISH procedure was carried out manually as per the manufacturer′s instructions. Slides were scored immediately using an Axio Imager Z1 (Carl Zeiss) upright fluorescence microscope equipped with appropriate excitation and emission filters allowing visualization of the signals, Axio Cam MRc5 camera, and Axio Vision Rel 4.5 software. The fields containing invasive tumor component with non-overlapping tumor nuclei were chosen for interpretation. A minimum of 40 tumor nuclei for each case were counted and only those nuclei showing at least one green and one red signal were selected. The total number of red and green signals counted in the tumor nuclei was recorded and then the ratio of the HER2 (red) to CEP 17 (green) signals for the 40 tumor nuclei was calculated. Other feature like polysomy 17 and genomic heterogeneity were also noted. Fields showing excess background signals or auto-fluorescence masking the nuclear signals were not evaluated. The interpretation of the FISH assay was done following the American Society of Clinical Oncology/College of American Pathologists (ASCO/CAP) guidelines. [7] A recounting of additional 20 tumor nuclei (i.e. total 60) was done for the equivocal cases. The assay was repeated in the case of failure of test due to technical problems, viz. excess paraffin in the tissue, excess background auto-fluorescence, no signal or improper protease digestion. Normal and amplified control slides, ProbeChek, were run simultaneously with the test cases. The slides were then stored in the dark at -20 o C. The statistical analysis consisted of a descriptive reporting of the percentages in various subgroups of patients. Proportions were compared using the chi square test. Results Patient profile and receptor expression A total of 2001 new patients with invasive breast cancer were diagnosed in our hospital in the year 2008. The baseline characteristics of the patients are shown in [Table - 1]. The median age of these patients was 49 years (range 20-99 years). The majority of patients were in the age group 35-70 years (n=1747, 87.3%). Invasive ductal carcinoma was the most common subtype (n=1908, 95.4%). The other subtypes were uncommon and are shown in [Table - 1]. Most of the tumors were Grade III (n=1508, 75.4 %). The ER, PR, and HER2 expression status of our patients is shown in [Table - 2]. ER/PR status was not available in 75 patients (3.7%) while HER2 data was missing in 79 (3.9%). This was because many of the tumor blocks were referred from outside and had poor preservation or insufficient material. The pattern of receptor expression in all patients is shown in [Table - 2]. Endocrine responsive tumors i.e. those expressing ER and/or PR comprised 51.2% (n=1025) of all invasive carcinomas. Of these, the majority of patients (n=752, 73.4 %) expressed both ER and PR. Triple negative breast cancers, defined as lack of expression of all three receptors, comprised 29.8% (n=596) of all invasive cancers. The number of patients with IHC HER2 3+ expression was 335 (16.7%) and those with HER2 2+ expression was 163 (8.1%) [Table - 3]. We also analyzed the receptor expression by the age of the patients [Table - 4]. HER2 over-expression was not significantly different in the age groups <35 years and 35-70 years (17.7% vs. 17.0% respectively, P= 0.825), it was also not significantly different in women older than 70 years compared to those in the 35-70 year age group (10.42% vs. 17.7%, P= 0.120).Triple negative breast cancer was more common in patients less than 35 years compared to those in the age group of 35-70 years (41.8% vs. 29.3%, P= 0.001) and less common in women older than 70 years compared to those in the age group 35-70 years (18.8% vs. 29.3%, P= 0.027). The rate of hormone receptor positivity (ER and/or PR positive irrespective of HER2 status) was higher in women older than 70 years compared to those between 35-70 years (76.0% vs. 51.3%, P= 0.0001) and lower in women younger than 35 years compared to those between 35-70 years (35.4% vs. 51.3%, P= 0.0002). The trend for receptor expression by age groups defined in decades is shown in [Figure - 1], which shows that ER and/or PR expression increases and triple negative phenotype decreases with increasing age. It is also interesting to note that all male breast cancers were hormone receptor-positive (22/24, data on receptor status not available in two male patients). There were no triple negative cancers and there was only one patient with HER2 IHC 2+ among the males. Among the 43 lobular carcinomas, 42 were HER2-negative and HER2 status not available for one. All patients with HER2 2+ expression in IHC do not undergo FISH testing at our centre because of financial constraints. Only those HER2 IHC 2+ patients for whom HER2-targeted therapy is feasible undergo FISH testing. From this data, therefore, it is not possible to ascertain the exact fraction of IHC 2+ patients in whom HER2 is amplified by FISH. However, in another study from our institution, performed during the same time period, 65.3% of IHC 2+ tumors had HER2 amplification by FISH. [8] Thus extrapolating the latter result to our group, the approximate number of HER2-positive patients would be 441 (335 patients with IHC 3+ expression plus 65.3%% of 163 IHC 2+ patients, i.e. 106). The use of HER2-targeted therapy These 441 patients (in all stages) were potentially eligible to receive HER2-targeted therapy as per current international guidelines. From the collected information we could ascertain that 38 patients (8.61%) received some form of HER2-targeted therapy. Of these 38 patients 20 (4.54 %) received HER2-targeted therapy (trastuzumab, lapatinib or neratinib) as part of ongoing approved studies at our institution, 12 in adjuvant and 8 in metastatic setting [Figure - 2]. The other 18 (4.08%) patients received HER2-targeted therapy (trastuzumab) as part of routine care, 16 in adjuvant and 2 in the metastatic setting. In the adjuvant setting patients received trastuzumab for either 12 weeks (as a modified FINHER type of protocol) or one year. Of the 18 routine care patients, 5 patients were recipients of some form of government-initiated health scheme or private insurance while the other 13 patients were self-financed. Discussion We report here the receptor expression profile of breast cancer patients presenting to a large cancer hospital in India in one calendar year (2008) and the use of HER2-targeted therapy in this cohort. This data has several strengths including the large number of patients and the uniform performance of pathological evaluation on tumor specimens by experienced oncopathologists in a high-quality laboratory. There are several points of note in this data that are different from the corresponding Western literature. The median age of our patients (49 years) is approximately a decade younger than the West. [9] This is likely to be due to the different age distribution of the Indian population, where only 7% of the population is above the age of 60 years. [10] The proportion of tumors with various patterns of receptor expression is different from that reported in the Western literature. The overall receptor expression pattern in our patients suggests a lower fraction of endocrine receptor-positive, higher fraction of triple negative and similar fraction of HER2-positive disease compared to the Western data. [2],[11],[12] Older patients (> 70 years) had a higher proportion of hormone receptor-positive tumors compared to others, suggesting that the lower overall fraction of endocrine receptor positivity may be due to the lower average age of our patients. Our data also suggest that very young patients (< 35 years) have a higher chance of having breast cancers with the triple negative phenotype compared to older patients. A tertiary care centre in south India has also recently reported a high percentage of triple negativity (25%) in their breast cancer patients (compared to the West) and a similar percentage of patients (27%) with HER2 positivity. [13] Another centre in India has reported a higher incidence of HER2 positivity by IHC (43.2%) although that by genomic polymerase chain reaction (PCR) in the same dataset was 25.5%. [14] The possible reason for this discrepancy is not clear. One possible explanation could be the fact that while 55 samples for PCR were consecutive in the period 2004-2005 in that data, IHC was also analyzed on an additional 313 blocks that were available from 1999-2002, possibly leading to bias. As we have reported above an estimated 441 patients were eligible to receive HER2-targeted therapy in the year 2008 in our institution. However, only 8.61% of these patients were able to receive such treatment and nearly half (4.54%) of the HER2-targeted therapy was through patient participation in clinical trials. The low usage of a highly effective treatment is ascribed to the financial constraints that are common in our patients and a healthcare delivery model wherein the majority of patients have no access to any form of health insurance. This is not unexpected in a country where the reported annual per capita income is INR (2009-10) 40,745 (approximately USD 1000). [15] The cost of one vial of trastuzumab (440 mg) is around INR 100,000 (approximately USD 2000). It should be noted that our institution is a publicly funded hospital that caters to all sections of the society including the economically disadvantaged ones. Therefore this data may not be reflective of the use of HER2-targeted therapy in private Indian hospitals that largely cater to economically stronger sections of the population. However, we believe that since the overwhelming majority of the Indian population in uninsured, has low annual income and resides in rural and semi-urban areas, our data accurately reflects the reality of low usage of effective but expensive anticancer treatments. It is important to initiate action on various fronts to improve this situation. This may involve reduced and realistic pricing of targeted anticancer drugs and wider coverage of the population by affordable insurance. It also calls for research efforts to develop accurate biomarkers of benefit and non-benefit from targeted therapies. As an example, approximately 60% of patients with HER2-positive early breast cancer will never relapse despite not receiving HER2-targeted therapy, which is evident from the control arms of the randomized trials. [5] It would be immensely useful to develop biomarkers that could segregate such patients with high predictive value. Lastly, ongoing trials that are evaluating shorter courses of adjuvant HER2-targeted therapy will be very useful in increasing the accessibility of these drugs, if shorter schedules were proven to be equi-efficacious to the prolonged ones. Cost-effectiveness studies show that the cost per life year gained is significantly less for the shorter duration courses. [16] This study has some weaknesses. The stage distribution of patients was not analyzed in the study. The reasons for non-use of HER2-targeted therapy have not been analyzed in detail. FISH for amplification of HER2 receptor was not performed in all IHC 2+ cases because of reasons mentioned above. Nevertheless, we believe that the present data are a reasonably accurate estimate of the use of HER2-targeted therapy in our institution and other parts of India. In summary, our data show that a lower proportion of Indian breast cancer patients have hormone receptor-positive and a higher fraction have triple negative phenotype compared to Western populations. These differences could, at least partly, be explained by the lower average age of our patients. A very small fraction of eligible patients is able to receive HER2-targeted therapy because of financial reasons. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11114t2.jpg] [cn11114t1.jpg] [cn11114t3.jpg] [cn11114f1.jpg] [cn11114f2.jpg] [cn11114t4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}