 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
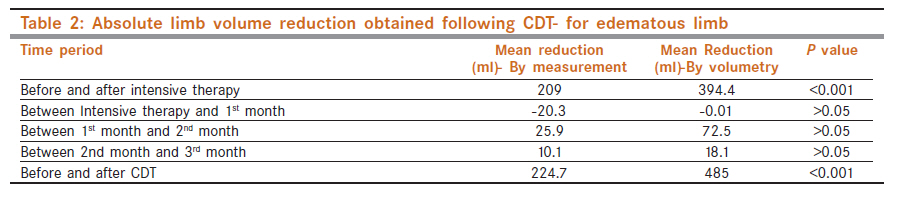
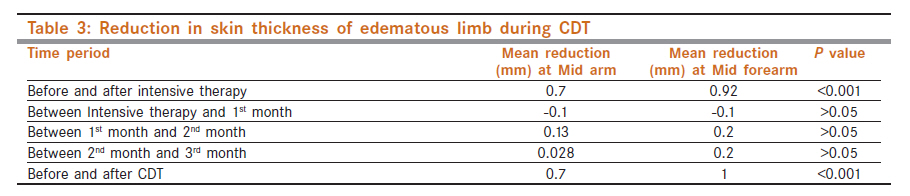
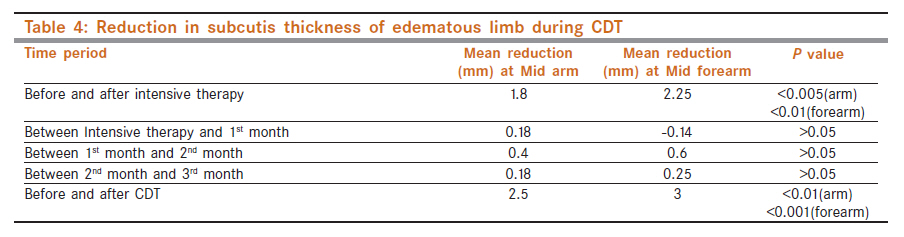
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 397-402 Breast - Original Article Comprehensive decongestive therapy in postmastectomy lymphedema: An Indian perspective S Randheer1, D Kadambari1, K Srinivasan1, V Bhuvaneswari2, M Bhanumathy3, R Salaja3 1 Department of Surgery, JIPMER, Puducherry, India Code Number: cn11115 PMID: 22293250 Abstract Background: Lymphedema following breast cancer treatment is one of the most morbid conditions affecting breast cancer survivors. Currently, no therapy completely cures this condition. Comprehensive Decongestive Therapy (CDT), a novel physiotherapeutic method offers promising results in managing this condition. This therapy is being widely used in the West. Till date, there are no studies evaluating the effectiveness and feasibility of this therapy in the east. Keywords: Comprehensive decongestive therapy, manual lymphatic drainage, volumetry Introduction Postmastectomy lymphedema is one of the most morbid conditions occurring after breast cancer therapy, causing severe physical, functional, and psychological distress to the patient. With improvements in breast cancer therapy, more women become long time survivors and hence the long term postoperative complications and their management become an increasingly important issue. [1] Postmastectomy lymphedema is a treatment related complication resulting from axillary surgery and radiotherapy. Even with less extensive axillary surgery and improved radiotherapy techniques, the literature reported incidence of this condition is about 12−54%. [2],[3],[4],[5],[6] Though not life threatening, it causes high morbidity with functional impairment and cosmetic disfigurement and has psychological effect on the patient, thus downgrading quality of life. Treatment of this condition poses a great challenge to physicians. Physical therapy is the mainstay of management. Pharmacotherapy and surgery give disappointing results. [6] A novel form of physiotherapy called Comprehensive Decongestive Therapy (CDT), which combines various physiotherapeutic modalities like massage, compression bandaging and exercises, is the standard therapy in some Western countries. [7] With over 150 mastectomies conducted every year in our institute, postmastectomy lymphedema is a major problem that many of our breast cancer survivors are facing. This study was undertaken to evaluate the efficacy of CDT in our patients. Patients and Methods This was a prospective study conducted on patients with post mastectomy lymphedema, attending the Cancer follow-up Clinic of our hospital from November 2006 to June 2008. A total of 35 patients presented with clinical evidence of lymphedema during the study period. Women with symptomatic or asymptomatic lymphedema that developed after a period of at least four months after completion of breast cancer treatment were enrolled in the study. Edema occurring within the first few months of therapy tends to be temporary and may subside without therapy. Those with a difference in volume between the two arms of less than 200 ml and a difference in circumference between the two arms of less than 2 cm were excluded. Women with evidence of locoregional recurrence of carcinoma, bilateral breast cancer and edema due to other causes (filariasis, primary lymphedema, and deep vein thrombosis) were also not eligible. Seven patients were excluded - two with local recurrence, one who had carcinoma in the opposite breast, two with metastatic disease, one due to recurrent cellulitis following bandaging, and one who had edema less than 200 ml; three patients were lost to follow-up. Lymphedema was staged using parameters such as pitting and dermal changes (skin thickening, skin folds, and papillomas) [Table - 1]. [8] The scar was examined for evidence of dense fibrosis and puckering indicative of severe postoperative infection or postradiation reaction. Objective assessment of lymphedema was done by measuring limb volume using multiple circumference measurements of the upper limb and by water displacement volumetry. The limb volumes of both upper limbs were measured. In circumference measurement method, the upper limb was divided into four segments. The upper limit of measurement, known as the 65% point, was a point marked on the upper arm, which is 65% of the distance from the olecranon to the acromion tip. The four segments were: (a) Wrist (at the level of ulnar styloid) to mid forearm, (b) Mid forearm to elbow (at the level of olecranon), (c) Elbow to mid arm and (d) Mid arm to the 65% point. Each of these segments was assumed to be a truncated cone (frustum). As the shape of upper limb is not exactly cylindrical, studies have shown that calculations using the frustum assumption produce the least standard error of measurement. [9] The volume of each segment was calculated using the formula, h (C12 +C22 +C1C2) / 12π, where h is the length of each segment, C1 and C2 are the circumference of each segment at both ends. The sum of these volumes gives the volume of the limb. In water displacement volumetry, the patient′s upper limb was immersed in a graduated steel cylinder up to the 65% point. The volume of water displaced was calculated using the formula πr2 h; where r is the radius of the cylinder and h is the height of water displaced. A graduated steel cylinder with an inner diameter of 38 cm was used in this study. Following this, the skin and subcutis, thickness of the upper limb were measured using high frequency ultrasound probes (10 MHZ). The measurement was made with the patient in sitting position with arms extended and measurements were made at anterior, posterior, medial and lateral aspects of mid arm and mid forearm and the average taken. Compressibility of axillary veins of both sides was assessed, to rule out axillary vein thrombosis. Following the initial assessment patients were started on the intensive phase of CDT, in the Physiotherapy Department. The intensive therapy was given four times a week (on alternate days), for two weeks. The patients were given Manual Lymphatic Drainage (MLD) for a period of 45 minutes, as per the Vodder technique. This was followed by multilayered compression bandaging of the upper limb, which includes finger bandaging, a gauze layer, a layer of foam, cotton wool pad, and an outer layer of low stretch elastic bandage (Top Grip™) of size 15 cm(w) × 4 m(L). The bandage was applied from the hand to the upper arm. The patients were also advised on skin and nail care and isotonic exercises to be performed with the bandages on. They were also advised to re-apply the bandages on the next day. After completion of intensive phase, the patients were assessed for reduction in limb volume using circumference measurements, displacement volumetry and sonographic measurement of skin and subcutis thickness. They were advised to massage themselves twice a day after performing deep breathing exercises. Other measures included isotonic limb exercises thrice a day, skin and nail care and application of low stretch compression bandages throughout the day and limb elevation at night. The patients were followed up monthly over a period of three months for assessment of reduction in limb volume. For each patient, the therapeutic response was calculated as the change in absolute limb volume (in millilitres) and as the change in excess volume of the treated limb before and after the intensive phase and at each month of follow up. The volume of edema was calculated as the difference in limb volume between the edematous and normal limb. Results were expressed as the percentage reduction in edema of the diseased limb, which was calculated as: Ethics This study was approved by the Institute Ethics Committee Repeated measures ANOVA was used to test the significance of difference in the absolute limb volume changes, the reduction in the amount of edema and the changes in skin and subcutis thickness before intensive phase, after intensive phase, at 1 st, 2 nd , and 3 rd months of follow up. A P value of less than 0.05 was considered significant. Correlation of the limb volumes assessed by measurement and volumetry was calculated using Pearson correlation. Statistical analysis of the data was done using GraphPad Instat 3 and SPSS 16.0 software. Results The mean age of the study group was 52 years; the range being 30-76 years. Majority of patients (72%), had T2 or T3 disease and 60% of patients had nodal involvement. All patients underwent total mastectomy with level II axillary dissection. About 92% of patients received neoadjuvant and adjuvant chemotherapy and post operative radiotherapy. Two patients did not receive radiotherapy of which one defaulted and the other was not given radiotherapy or chemotherapy in view of advanced age and early stage of disease. As much as 28% of patients had history of postoperative wound infection and 24% of patients had a puckered scar on examination, indicative of a severe postoperative infection or radio dermatitis. The median time for development of lymphedema was six months following surgery or radiotherapy. The two patients who did not receive radiotherapy developed lymphedema two months and 26 months after surgery. Majority of the patients presented with stage I lymphedema (92%). The most common symptom was heaviness of the affected limb (76%). 76% had right-sided lymphedema, as majority of patients had right sided breast cancer. All patients were right handed. The mean volume of the edematous limb in the study group, before treatment, was 2603±687 ml, by circumference measurement and 3296±988 ml by volumetry vs 1848.3±320 ml, by measurement and 2144.4±430 ml, by volumetry in the normal limb. The mean skin thickness at the mid arm and mid forearm levels for the edematous limb was 2.8±0.9 mm and 3.04±1.2 mm, respectively, and for the normal limb was 1.5±0.3 mm and 1.4±0.28 mm, respectively. The mean subcutis thickness at the mid arm and mid forearm levels for the edematous limb was 14.9±4.4 mm and 11.9±5.4 mm, respectively, and that for the normal limb was 9.6±3 mm and 5±1.5 mm, respectively. During analysis of data, it was observed that on applying the tests of normality (Kolmogorov- Smirnof test) the data were not normally distributed (positively skewed). Hence, log transformation of the data was done before analysis. With CDT, the mean reduction in absolute limb volume of the edematous limb was 224.7 ml by measurement and 485 ml by volumetry (P<0.001). The maximum reduction in volume was observed after the intensive phase of therapy [Table - 2]. The percentage of lymphedema, which is the amount of edema expressed as a percentage of the normal limb volume, reduced from 55.7% to 31% (P<0.01) after the therapy. The reduction in limb volume observed after therapy was 32.3% and 42% of the excess, by measurement and volumetry, respectively However, two patients did not show any improvement with therapy and had an increase in volume of 320 ml and 146 ml by measurement. No change in volume was recorded by volumetry. One of them had fungal infection of the skin and was less compliant to therapy, and the other patient was non compliant to the maintenance therapy and was on irregular follow up. In the maintenance phase, it was observed that there was a mean increase in limb volume by 20.3 ml, which was not statistically significant (P>0.05). Even though there was a reduction in limb volume on subsequent follow ups at second and third months, the reductions were not statistically significant (P>0.05). However, the overall reduction in limb volume before and after therapy was found to be significant; P<0.001 [Table - 2]. The reduction in skin and subcutis thickness of edematous limb during therapy followed almost the same pattern as the volume reduction. [Table - 3], [Table - 4] There were no significant changes in the volume or skin and subcutis thickness of the normal limb, before and after therapy. The response to therapy was not influenced by factors like preoperative nodal status, presence of post operative infection, puckered scar or the side of involvement. Two patients developed skin irritation and blistering following application of multilayered bandaging. Of this, one patient responded to conservative management and continued the therapy without further complications, while the second patient had severe blistering and was excluded from the study when she developed distant metastasis. One patient developed recurrent episodes of cellulitis following bandaging, during the maintenance phase and hence was excluded from the study. One patient presented with recurrence of lymphedema one year after therapy, due to non compliance to the maintenance therapy. It was also observed in the study that the measurements by volumetry and circumference measurements had a correlation coefficient of 0.98. Discussion Postmastectomy lymphedema is a significant long term problem for breast cancer survivors. Although the incidence of this condition has decreased recently with the advent of more conservative approaches in surgery like breast conservation surgery and sentinel lymph node biopsy, literature reports an incidence of 12−54% for this condition. [2],[3],[4],[5],[6] As there is no treatment that can offer cure for this condition, management is challenging. Treatment for lymphedema can only aim to control rather than to cure. [7] At present, multimodal physical therapy is the standard of care. [10] The goals of lymphedema management are to prevent the progression of the disease, to reduce and maintain the limb size, to alleviate symptoms, to improve mobility and ability to perform daily activities, and to improve overall psychological well being. Comprehensive Decongestive Therapy (CDT), a multimodal therapy, comprising of manual lymphatic drainage (MLD),compression bandaging, exercise, skin and nail care, is a promising way to treat all forms of lymphedema. Irrespective of the stage of lymphedema, etiology, or medical co morbidities, most lymphedema patients are treated in a comparable fashion by CDT. [11] Relatively few studies exist evaluating the effectiveness of this therapy. Till date, no studies on CDT have been reported from the Indian sub continent. This study showed a reduction in the absolute volume of the edematous limb by 485 ml. The maximum reduction was obtained after the intensive phase of therapy. The lymphedema reduction averaged 34% after the intensive phase of therapy and 42% at the end of three months. The amount of edema reduced by 244 ml after three months of therapy. The results obtained in this study are comparable to the results of other studies. [12],[13],[14],[15] Andersen and Hamner et al. reported an average reduction of edema by 298 ml and 237 ml after the intensive phase, respectively. [13],[14] The percentage reduction of edema obtained in these studies was 44% and 42%. As observed by Andersen, [13] though the volume reduction could be maintained during the follow-up period, there was some loss of the initial lymphedema reduction obtained after the intensive phase. This loss of the initial reduction can be attributed to the non compliance of the patients to the maintenance phase. In our study, it was observed that in the first month of follow-up, nineteen patients had some loss of the edema reduction achieved after the intensive phase. It was found that these patients did not strictly follow the bandaging and simple lymphatic drainage protocols. Nearly eighty percent patients were non compliant to bandages, owing to the discomfort of using them in the hot climate, and due to interference with their day-to-day activities. Most of the patients were found to have forgotten the sequence of massage to be followed in simple lymphatic drainage, during the maintenance phase. During each follow-up, patients were motivated to continue their bandaging and the steps of simple lymphatic drainage revised. It was observed that patients followed the maintenance phase protocols better on motivation, which was reflected by small reductions in edema during further follow-ups. However, the overall compliance to bandaging was less owing to the discomfort the patients experienced while wearing them in the hot climate and in doing their daily routine. Although compression sleeves are more user friendly, due to the ease of application and less discomfort, they are too expensive. Thus, compliance to bandaging and massage during the maintenance phase was a very important factor in maintaining the reduction obtained during the intensive phase and for further reductions thereafter. [15],[16] Boris reported that non compliant patients had their reductions worsened from 63% to 43%. [15] Mellor reported that skin thickness measurement using high frequency ultrasound was a simple and reliable method to assess lymphedema and to investigate therapeutic interventions. [17] However, there are no studies on the use of ultrasound measurement in assessing the response to CDT. It was observed in this study that changes in skin and subcutis thickness followed the same trend as volume changes, during the course of CDT. The volumes assessed by volumetry and circumference measurement showed a mean difference of 690 ml for the edematous limb and 298 ml for the normal limb. This discrepancy can be explained by the fact that in volumetric measurement the volume of the entire upper limb was calculated, including that of the hand, as the whole upper limb was immersed in the cylinder of water. In circumference measurement method, the volume of the hand was excluded, as the measurement started at the level of the wrist. Sander et al. reported a difference of 479 ml to 665 ml between volumetric and geometric measurements of the arm. [18] Karges reported a mean difference of 96 ml between these two methods, when the volume of fingers was excluded from the volumetric measurements. [19] Both studies reported a high correlation between the volumes calculated by geometric measurements and volumetry, which was also demonstrated in our study (r=0.98). However, studies have shown that the differences between the two methods are too large to substitute measurements made with one method for the other. One of the methods can be reliably used for assessing the volume for clinical and research purposes. [18] The limitations of the study were the small sample size and shorter duration of follow up, when compared to similar studies. Another drawback was that the improvement in the quality of life of patients was not assessed. A standard volumeter was not used in the study, and hence the hand volumes could not be measured accurately, so as to exclude them from the limb volumes measured by volumetry. This study showed that comprehensive decongestive therapy can effectively promote acute limb volume reduction in patients with post mastectomy lymphedema, and when combined with self care results in long term control of lymphedema. One of the problems faced by patients in a tropical country like India is the discomfort due to bandages. The hot climate and the associated perspiration might be the cause for intolerance to bandaging seen in some patients, manifested by repeated episodes of cellulitis, blistering, and exacerbation of fungal infection. However, literature, which is mostly from the Western world, has not reported any such complications associated with this therapy. The climatic conditions in the tropics are thus an important factor that adds to the non compliance to this therapy in our population. Emphasis on proper skin care and devising an alternative component to continuous bandaging like Intermittent Pneumatic Compression may be helpful to combat the complications as well as the non compliance to bandaging, especially for patients in tropical countries. Conclusions CDT, when combined with long-term self management proves effective in controlling postmastectomy lymphedema. Patient compliance to treatment protocols like regular manual lymphatic drainage, compression bandaging, skin, and nail care is very important in achieving and maintaining reduction in limb volume following therapy. The hot climate in tropics is a factor that limits the regular use of compression bandages by the patients and may be responsible for the intolerance to bandages as evidenced by recurrent cellulitis, blistering, and exacerbation of fungal infections seen in some patients. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11115t3.jpg] [cn11115e1.jpg] [cn11115t4.jpg] [cn11115t1.jpg] [cn11115t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}