 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
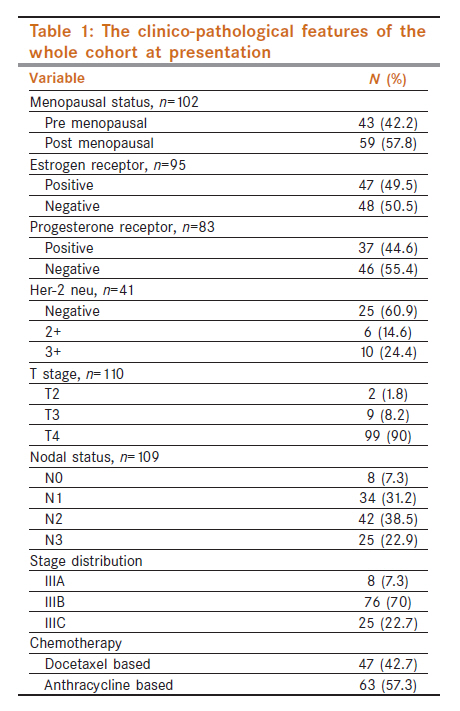
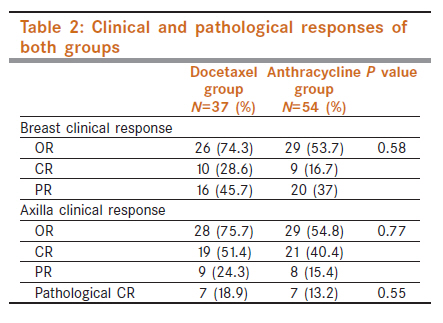
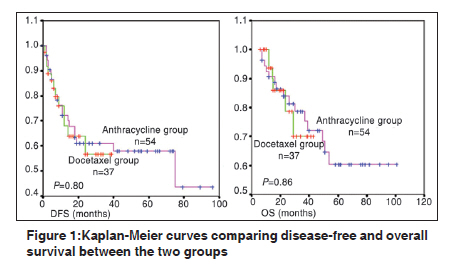
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 410-414 Breast - Original Article Clinical and pathological response rates of docetaxel-based neoadjuvant chemotherapy in locally advanced breast cancer and comparison with anthracycline-based chemotherapies: Eight-year experience from single centre D Gupta1, V Raina1, GK Rath2, NK Shukla3, BK Mohanti2, DN Sharma2 1 Department of Medical Oncology, Bhagwan Mahaveer cancer Hospital & Research center, Jaipur, Rajasthan, India Code Number: cn11118 PMID: 22293253 Abstract Introduction: The administration of neoadjuvant chemotherapy (NACT) prior to local therapy is advantageous for women with locally advanced breast cancer (LABC), since it can render inoperable tumors resectable and can increase rates of breast conservative surgeries. Keywords: Docetaxel, locally advanced breast cancer, neoadjuvant chemotherapy Introduction Breast cancer is the most common cancer in females with age-adjusted incidence rates of 124 /1,00,000 population in the USA. [1] In India approximately 75-80,000 new cases are diagnosed annually. [2],[3] The Annual Age Adjusted Rate (AAR) varies in urban population based cancer registries from 27.0 per 100,000 in Chennai to 33.4 per 100,000 in Delhi while in Barshi it is 7.2 per 100,000 population. [4] Locally advanced breast cancer (LABC) accounts for 30-60% of breast cancer in developing countries while in USA it accounts for 10-20%. [5] LABC refers to large breast tumors (>5 cm) associated with either the skin or chest wall involvement or with fixed axillary lymph nodes or disease spread to ipsilateral internal mammary node or supraclavicular node. [6] First report of the use of neoadjuvant chemotherapy (NACT) for LABC was published in the 1970s. [7] The administration of systemic chemotherapy prior to local therapy is advantageous for women with LABC since it can render inoperable tumors resectable and can increase rates of breast conservative surgeries. [8],[9],[10],[11] Induction chemotherapy also has a theoretical advantage of early initiation of systemic therapy and delivery of drugs through intact vasculature. Anthracycline-containing regimens are the standard of care and known to be highly active in the treatment of breast cancer and therefore are predominantly being used in the treatment of breast cancer. Taxanes are emerging as effective chemotherapy drugs in breast cancer. Neoadjuvant use of paclitaxel alone or in combination has been shown to result in superior response rates compared to anthracycline-based chemotherapy. [12] Docetaxel has been an extensively studied molecule in the treatment of breast cancer, either alone or in combination, and has been shown to produce higher response rates then anthracyclines alone. [13],[14],[15],[16],[17] At our institute, a docetaxel-based NACT combination is being used in the treatment of LABC since 2004. We analyzed the data of those LABC patients who received docetaxel based NACT to assess the clinical and pathological response rates, disease-free survival, overall survival and to compare the results with that of anthracycline-based regimens historically. Material and Methods We screened case records of all registered breast cancers from January 2000 to December 2007 and clinically staged LABCs with confirmed histopathological diagnosis were selected for analysis. Those patients who had received prior chemotherapy/radiotherapy were excluded. Baseline information regarding demography, clinical stage, hormone receptor status, etc. was collected for all patients started on NACT while response assessment and survival analysis was restricted only to those patients who had received at least three cycles of chemotherapy and underwent definitive surgery. Data for clinical response rates, number of preoperative chemotherapy cycles, type of chemotherapy, pathological stage and pathological response rates was collected. Response rates, disease-free survival (DFS) and overall survival (OS) of patients receiving docetaxel were compared with those who received anthracycline based chemotherapy. Pathological CR was defined as no evidence of malignancy in both the breast and axilla. Overall survival was calculated from the date of diagnosis till last seen or date of death. Disease-free survival was calculated from date of surgery till either relapse or date of death or date last seen whichever was earlier. SPSS Version 11.5 software was used for statistical analysis. The t-test/Mann-Whitney test was applied wherever required to compare the continuous variables. For categorical variables, Chi square/Fisher′s exact test was used. Survival curves were generated using Kaplan Meier method and survivals compared with log-rank test. Ethical committee approval was obtained prior to analysis. Results Approximately 3000 case records were screened over eight years. There were 570 (19%) LABC patients. Only 110 chemo-naïve patients with confirmed diagnosis and started on NACT were eligible (47 in the docetaxel arm, 63 in the anthracycline arm) for baseline clinicopathological features and 91 (37 docetaxel, 54 anthracycline) patients who underwent surgery were eligible for survival analysis. Median age of the whole cohort was 45 years (range 25-68 years). Fifty-six (50.9%) patients had right-sided tumors while 54 (49.1%) patients had left-sided tumors. Thirty percent (12/40) patients were triple negative for all three hormone receptors. The clinico-pathological features at presentation are detailed in [Table - 1]. Chemotherapy regimens given in the docetaxel group comprised of docetaxel 75 mg/m², epirubicin 75 mg/m² and cyclophosphamide 500 mg/m² (DEC) and the anthracycline group received either doxorubicin 50 mg/m² or epirubicin 75 mg/m² along with 5-FU 500 mg/m² and cyclophosphamide 500 mg/m² (FAC or FEC respectively). Patients in the docetaxel group received median of six cycles of preoperative chemotherapy with 24 patients receiving six cycles, six patients four cycles and 17 patients received ≤three cycles. In the anthracycline group the median number of preoperative cycles were three, with 39 patients receiving three cycles, 17 patients receiving six cycles and three patients each received four and five cycles. Surgery performed was modified radical mastectomy (MRM) for all patients in both groups. Adjuvant treatment consisted of chemotherapy (remaining chemotherapy cycles) in 15 (40.5%) and 37 (69.8%) [P=0.009], radiotherapy in 31 (83.7%) and 50 (92.6%) [P=0.64] and hormone therapy in 20 (54%) and 38 (70.37%) [P=0.05] patients for the docetaxel and anthracycline group respectively. The response rates are depicted in [Table - 2]. Although pathological complete remission (pCR) rates were more in the docetaxel group, it did not reach statistical significance. There was no significant difference in pCR achievement when compared for estrogen receptor positive vs. estrogen receptor negative groups. Three-year DFS was 56.84% (median not reached) for the docetaxel group and 61.16% (median 75 months) for the anthracycline group. Three-year OS was 70% (median not reached) and 78.59% (median not reached) respectively with median follow-up of 19 months (range 6-43) and 32 months (range 7-101) respectively. There was no statistically significant difference for OS and DFS between the two groups (P=0.86 and 0.80 respectively) [Figure - 1]. Among patients who achieved pCR with NACT, only three patients relapsed and median DFS was not reached while 30 patients relapsed and median DFS was 75 months for those who did not achieve pCR, however, it did not reach statistical significance (P=0.34). Similarly, OS was not significantly different between those who achieved pCR vs. those did not achieve pCR (P=0.31). Therapy-related toxicities were not assessed because of poor documentation in case records but no significant grade 3 and 4 toxicities were recorded in both arms. Discussion Previous retrospective analysis of LABC from our institute showed that LABC comprises 26% of all breast cancer patients. [18] The median age was 48 years with 43% premenopausal and 63% ER+ tumors. In another study, Bines et al., analyzed LABC patients on NACT prospectively. In that study median age was 50 years with 47% premenopausal patients, 54% ER+ tumors, 21% her-2 positive and 64% were Stage IIIB tumors. In the current study, there were 19% LABC patients with similar demography and maximum patients were of Stage IIIB (70%). Pathological CR has been shown to be an independent predictor of prolonged DFS/OS but very few patients achieve pCR and that too is dependent upon the type of chemotherapy. [19] Earlier trials testing anthracyclines as NACT produced pCR rates of 2-13% and there was no difference in DFS/OS. [18],[20],[21],[22] Subsequently, taxanes have been used either alone or with anthracyclines and it has shown to improve pCR rates. Single agent docetaxel has produced pCR rates of 16-20% andnical complete responses of 18% to more than 25%. [13],[14],[23],[24] In combination with anthracyclines pCR rates of 10% to >20% are reported depending upon the stages of tumor included in that particular study. [17],[25],[26],[27],[28],[29] As most of the trials are retrospective, have small sample size and include a heterogeneous group of patients, it is not possible to directly compare the results but the pCR and cCR in our study are in accordance with results previously reported in the literature. Historically, NACT has not led to increased DFS/OS but achieving pCR is associated with longer DFS/OS. In a recent update of NSABP B-18 and B-27 trials, there was no survival advantage with NACT and addition of taxane to preoperative chemo did not translate into higher survivals although pCR rates were higher. [20],[30] In our study too there was no difference in survival between the anthracycline and docetaxel groups and we failed to demonstrate longer DFS/OS for those who achieved pCR vs. non-pCR achievers. There was heterogeneity in the two groups regarding the number of cycles administered before surgery. Most patients in the anthracycline group had received three cycles compared to six cycles in the docetaxel group. Although there is no optimum duration defined, recently the international expert panel recommended that preferably all NACT should be finished preoperatively and that at least four cycles should be given before surgery. [31] Steger et al., have shown an increase in pCR rates from 7.7% to 18.6% with six cycles compared to three cycles. [32] In our study the pCR rates with anthracyclines was 13.2% overall but when we analyzed only those patients who received six cycles before surgery, they had pCR of 15.3%. Although the results in our study are compatible with previous results, there are limitations of retrospective analysis. There is disparity in the number of patients, number of cycles administered before surgery and in the median follow-up of the two groups. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11118f1.jpg] [cn11118t1.jpg] [cn11118t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}