 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
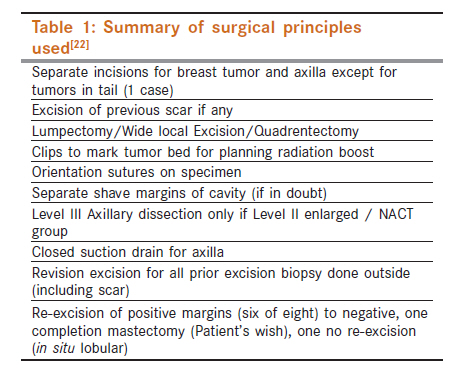
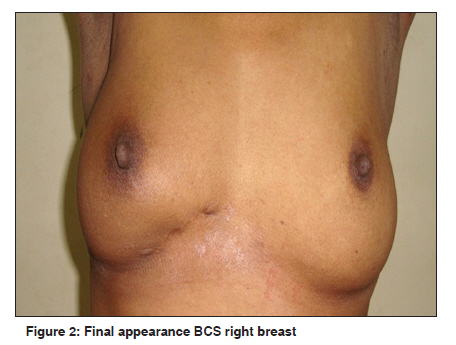
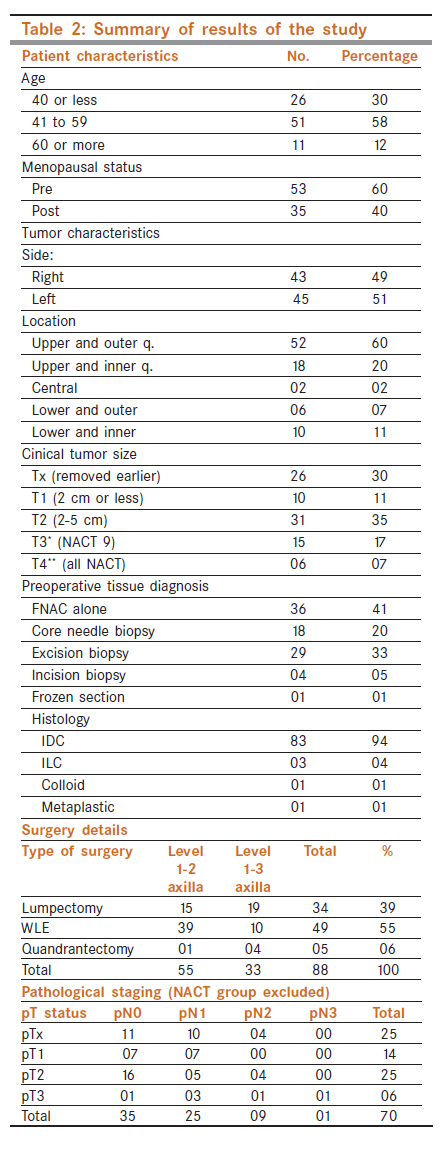
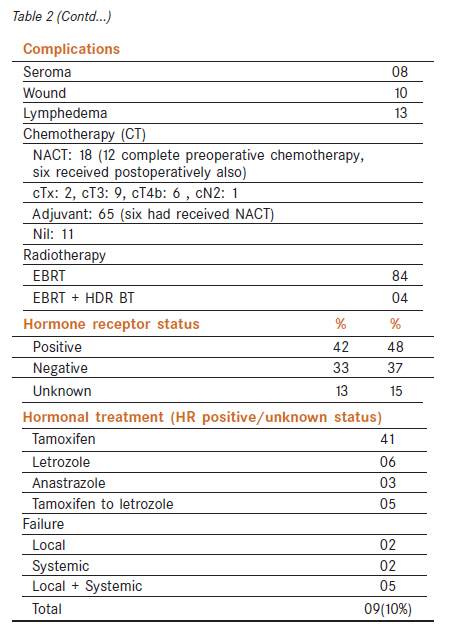
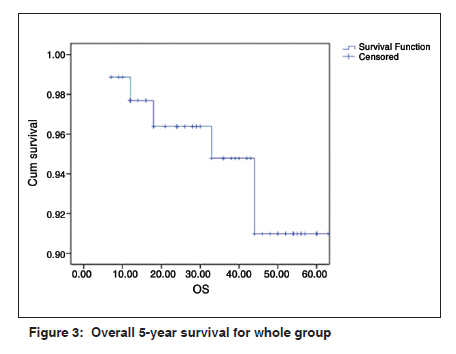
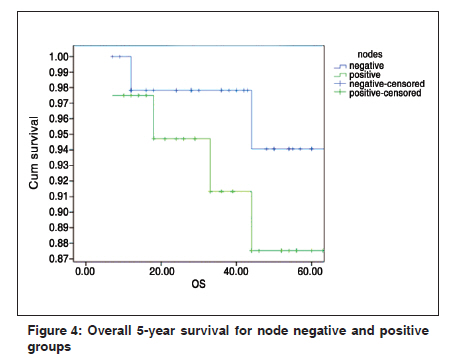
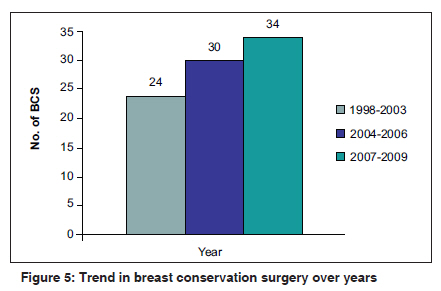
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 415-422 Breast - Original Article Breast conserving surgery for breast cancer: Single institutional experience from Southern India H Narendra, S Ray Department of Surgical Oncology, Kasturba Medical College, Manipal University, Manipal, India Code Number: cn11119 PMID: 22293254 Abstract Context: In India, breast conservation rates vary anywhere from 11 to 34%. This is in contrast to western world where breast conservation rates exceed 70% for early breast cancer. Keywords: Breast cancer, breast conservation surgery, breast conservation treatment Introduction Breast cancer has become the most common cancer among women in urban India (34% of all cancers). [1] Surgery for operable breast cancer has evolved a long way since W. Halsted first described radical mastectomy. In order to lessen the cosmetic and functional morbidity associated with classical radical mastectomy various modifications were described by Patey, Madden and Auchinclaus to name a few. Further, contributions from Keynes, Atkins et al, Mustakallio, Hayward, and others, firmly established the breast conserving techniques. [2],[3],[4],[5] Veronosi et al described their results of Quadrentectomy with axillary dissection and radiotherapy (QUART). [6] At present, most common surgical options for operable breast cancer are modified radical mastectomy (MRM) with or without reconstruction and breast conservation surgery (BCS). Choice of the procedure depends on various factors like surgeon′s training, patient′s desire, size of the tumor to breast ratio, the presence of contraindications for conservation and availability of radiotherapy facilities. At present, breast conservation treatment (BCT) comprises BCS and whole breast radiotherapy. The loco regional recurrence rates and overall survival (OS) rates with BCT are comparable to that of MRM. Based on the results of randomized trials conducted in Europe and North America in the 70s and 80s, BCT is the standard of care for early breast cancer in the west. [7],[8],[9],[10],[11],[12],[13],[14],[15],[16] But in India, BCT is not popular among the surgeons (11-23% vs. > 60-70% in west). [1] The advantages of BCS over MRM include better body image, sexual functioning and better psychological adjustment. [17],[18],[19] At our Institute BCT is being offered to breast cancer patients from the year 1997. Earlier indications were rigid, and isolated cases were offered breast conservation. The rate of breast conservation has gradually increased and at present, we offer neoadjuvant chemotherapy (NACT) and attempt to conserve breast in patients desiring so who meet all other criteria except for size. Studies from India with respect to outcome of breast conservation are sparse. There are also concerns regarding reproducibility of excellent results achieved in western women in Indian women owing to inherent differences in tumor stage, biology and quality of care. [20] At present, India is witnessing a sort of revolution in cancer care with the commissioning of newer treatment centers particularly in private sector; hence the rates of breast conservation are expected to increase. [21] Here we are reporting our experience with the BCS and BCT. Materials and Methods The study was conducted in a tertiary care university attached cancer hospital in South India. The study comprised of retrospective collection of prospective data of patients who underwent BCT until December 2009. All patients diagnosed with breast cancer were evaluated with bilateral breast mammogram, a chest X-ray, liver function tests including alkaline phosphatase and complete blood counts. Bone scan was done only for symptomatic patients or patients with elevated ALP or node positive patients. Once staging work-up is done, all patients were evaluated by a multidisciplinary team for suitability of BCT. Those with contraindications were excluded. Others were offered the option of either MRM or BCT. Those who desired conservation were included. The patients with larger tumors, desiring to conserve breast were offered NACT. The standard surgical principles described elsewhere were followed [Table - 1]. [22] Median follow-up period was 46 months (ranged from 7 to 154 months). After surgery all patients were referred to medical oncology/oncology services for decision regarding adjuvant chemotherapy. After completion of systemic chemotherapy all patients received 50-55 Gy of whole breast radiotherapy with a tumor bed boost of 9-12 Gy in daily 2 Gy fractions for 5 days in a week over 5-6 weeks. Four patients received HDR brachytherapy for tumor bed boost. After completing radiotherapy, hormonal treatment was initiated for patients with receptor positive or unknown status. Details like age, menopausal status, site and size of the tumor, histology, pTNM, adjuvant/neoadjuvant treatment, margin status, nodal yield, hormone receptor status, complications of treatment, locoregional and distant failures were recorded and disease-free survival (DFS) and OS calculated. Cosmetic outcome is being assessed as a part of another study. Median follow-up period was 49 months and mean 52 months (range 6-154 months). After completion of treatment, patients were called 3 monthly for first 2 years, and then every 6 monthly for follow-up. At each visit evaluation included detailed history, physical examination and symptom directed investigations. Post-BCT baseline mammogram was obtained 6 months to 1 year after completion of radiotherapy and annually thereafter. Women receiving tamoxifen were referred for annual gynecological examination [Figure - 1] and [Figure - 2]. Statistical methods The statistical analysis was performed using SPSS version 16 software for Windows. Local recurrence was defined as any histological or cytologically confirmed recurrence in the treated breast or overlying skin. DFS was defined as the period from date of surgery to local, regional or systemic relapse and overall survival as interval from date of diagnosis to death or last contact with the patient. Disease-free and cumulative survival curves were estimated using Kalpan-Meir survival analysis. A P-value of 0.05 or less was considered as a statistically significant. Results Total 88 patients underwent BCS during the study period. Total number of MRM during the same period was 80 in the department; hence BCS rate was 52%. Earlier to 2004, only 24 patients underwent BCS compared to 64 patients (71%) from 2004 to 2009 [Figure - 1]. Age range was 24-78 years (median age 45 years), 35 (40%) were postmenopausal and 53 (60%) were premenopausal. Most common tumor location was in the upper outer quadrant followed by upper inner quadrant [Table - 2a and Table - 2b]. Fine needle aspiration cytology (FNAC) alone was used to diagnose in 36 patients. Among the biopsy procedures, majority had excision, most of which were done elsewhere. Core needle biopsy was our preferred method of diagnosis. The most common histology was infiltrating ductal carcinoma, NOS type (83 of 88). Only three patients had invasive lobular carcinoma. Majority of the tumors were cT1/T2 category (41, 47%) and 23% of the tumors belonged to cT3/T4 category. Most commonly performed procedure was wide local excision (49 of 88 patients) followed by lumpectomy (34 patients) and quadrantectomy in five patients mainly in those achieving complete clinical response with NACT. Fifty-five (62%) patients underwent only level 1 and 2 axillary dissection and remaining 33 patients had complete (levels 1-3) axillary dissection. Average nodal yield was 11 (range 1-32), median 9, lower yield coming mainly from preoperative chemotherapy group. Majority had node-negative disease (48, 55%). Twelve of 18 patients who received preoperative chemotherapy had node-negative disease on final histology. Seventy-six patients (86%) achieved negative margins at first attempt and 12 had positive margins. Out of these 12, one opted for mastectomy and three patients refused re-excision, who were treated with higher radiation boost to tumor bed and rest eight had negative re-excision margins. Eighteen patients (20%) developed immediate postoperative complications, most common being wound related followed by seroma. Most of the wound-related complications occurred in patients receiving high-dose rate (HDR) brachytherapy for tumor bed boost. Hence this practice was discontinued in the latter part of the study. Apart from this, mild to moderate lymphedema of ipsilateral arm was a long-term complication in 13 patients (15%). Hormone receptors were positive in 42 patients; status was unknown in 13 patients. Postoperative chemotherapy was employed in 65 patients. Most common postoperative regimen used was four cycles of 3-weekly AC. Eleven patients (13%) did not receive any chemotherapy due to favorable tumor characteristics. Eighteen patients (20%) received NACT. Nine of the 15 patients with cT3 tumors received NACT for downsizing the tumor to allow for breast conservation. All patients with cT4b status received NACT. One patient had cT2N2; one had cTXN1 status and another one cTxN0. Twelve patients received complete course of chemotherapy preoperatively and most commonly used regimen was 3-weekly AC for four cycles followed by four cycles of 3-weekly paclitaxel. The most common complication observed was febrile neutropenia (five of six patients developing complications). Seven patients (39%) achieved pathological complete response (pCR) with NACT. After the completion of chemotherapy (if any) all patients received whole breast irradiation. HDR brachytherapy was used in four patients for delivering tumor bed boost. Local recurrence developed in seven patients (8%) out of which five patients also had systemic disease at the time of recurrence. Two patients developed systemic disease alone. The estimated overall 5-year survival was 91% for the whole group, 94% for node negative and 87% for node-positive patients (P=0.32, [Figure - 3] and [Figure - 4]). The 5-year DFS for whole group was 89%, 95% for node negative and 83% for node-positive group (P=0.25). On univariate analysis only factor found to have association with DFS was age less than 40 years (P=0.045). Discussion Breast conservation has become the standard of care in Western countries for early breast cancer. [8],[9],[10],[23],[24],[25],[26],[27],[28 ] In India BCT still not popular due to various reasons including advanced stage at presentation, cost of treatment, lack of appropriate equipments and facilities, physician′s and patient′s awareness. [1],[29],[30] In the recent years, many centers particularly in the private sector have come up with appropriate equipment and infrastructure facilities, which will influence the treatment and outcome of patients with breast cancer in India. Now, with the latest technology it is possible that every patient with breast cancer can have option of conserving breast which can have tremendous impact on her psychological and social health. [31],[32],[33],[34],[35],[36],[37],[38],[39],[40] Worldwide, trend to conserve breast has increased over years, which is also reflected in the present study as well as other studies from India [Figure - 5]. [30] Such a trend could be attributed partly to the early detection by widespread use of mammography. In the present study, the median age at diagnosis was 45 years, which is similar to other studies from India. This is almost a decade younger than western population. It is interesting to note that almost one third of the patients were younger than 40 years of age [Table - 1]. This probably reflects a preference towards opting for BCS in this particular age group. [20] Most women were premenopausal. Majority of the breast cancers were diagnosed by FNAC alone. It has been our departmental policy to rely on FNAC report for all patients undergoing BCS as against MRM. Majority of the excision biopsies were done elsewhere. Our policy has been to perform core needle biopsy if considering NACT before BCS. Three procedures done for the primary tumor included lumpectomy, wide excision or quadrantectomy. The quandrantectomy was done mainly in those who achieved complete clinical response following NACT. The local recurrence rate at a median follow-up period of 49 months was 7%. Only 2 patients had isolated local recurrence which could be surgically salvaged. Other five patients had developed systemic disease at the time of local recurrence. This emphasizes the concept that, type of local treatment rarely determines the OS. Hence attempts are being made by various investigators to avoid axillary dissection even in node positive patients. The local recurrence after BCS can be classified as either true occurring within the vicinity of tumor bed or false which are actually new or second primaries. Most of the true recurrences occur within 2 years of completing the treatment. The factors known to increase the risk of local recurrence include young age, status of resection margin, presence of extensive intraductal component and the lymph node involvement. [6],[41] But in the present study as the total number of events was small, we could not find any statistically significant association. Nearly 30% of patients in the present study were younger than 40 years of age and local recurrence rate in this subgroup was only 5%. But four of the seven local events occurred in this subgroup. Another potential problem in the young population is the risk of developing second primary in the conserved or contralateral breast. [42],[43] The reported complications of breast cancer surgery include seroma and lymphedema. Complication rate in the present study was 23%. Higher rates are probably influenced by the wound breakage in patients receiving high-dose brachytherapy in the early part of the study. Several studies have reported overall complication rates of 10-30 %. [44],[45] The success of BCT largely depends on cosmetic outcome and patient′s perception about conserved breast. Poor cosmetic outcome which is directly associated with the volume of breast excised, can jeopardize the main goal of conservation. After BCS, breast asymmetry can be a major concern. Poor cosmetic outcome could broadly be due to the patient or treatment-related factors. In one of the studies, looking into these factors, important patient-related risk factors were younger age, larger body habitus, larger tumor size, and tumor position, specifically superior medial tumors and inferior lateral tumors. The treatment related risk factors for postoperative asymmetry included tumor re-excision, seroma and breast irradiation. The need for re-excision after initial lumpectomy was associated with more breast asymmetry. By employing emerging oncoplastic and reconstructive techniques, one can overcome the poor cosmetic results. [46],[47],[48] In the present study patient satisfaction was good or excellent in more than 90% of the time. Detailed cosmetic evaluation is being assessed as a part of another ongoing study. Owing to the lack of nuclear medicine facilities, in majority of the Indian hospitals, routine level 2 axillary dissection has been the most widely used staging procedure for axilla. Sentinel node biopsy for clinically negative axilla has been the standard elsewhere. In order to reduce the morbidity, avoiding axillary dissection in sentinel node positive axilla has been current topic for the debate. [49] Neoadjuvant therapy can expand the indications for breast conservation. [50] By downsizing the large tumor it allows for BCS. In the present study nearly 19% of the patients received NACT and then underwent BCS. pCR was 39%. The majority of those achieving complete clinical response underwent quadrentectomy. Routine prechemotherapy tumor localization with metallic clips or slow clearing dyes can aid breast conservation in this setting. [51],[52] The reported pCR rates vary between 3 and 34 %, rates are higher when the complete course of chemotherapy is completed before surgery. [53],[54],[55],[56],[57],[58] Postoperatively, majority of the patients received adjuvant chemotherapy. Hormonal treatment was employed for receptor positive or status unknown patients. Radiotherapy is an integral part of the BCT. Several recent trials suggest that this can safely be omitted in a few selected patients such as elderly women with the hormone receptor-positive tumors less than 5 cm. [59],[60],[61] At present whole breast radiation is the standard of care. Various attempts at partial breast radiation are being considered in various trials. The results of these trials can change approach in coming years. Complications of radiotherapy such as dermatitis, edema, fibrosis and scarring can bring down the cosmetic outcome of BCS and can also interfere with the early detection of local recurrence. Finally, acceptability of BCS depends apart from the patient′s educational and economic background, also on the treating surgeon′s training. Several studies suggest that most women prefer BCS over mastectomy when given a choice. [62],[63] If eligible women are not given the option of conserving breast, naturally BCS rates will be lower. The present study highlights the acceptability of BCS in Indian women, when given as an option for patients with operable breast cancer as well as its equivalence with mastectomy in terms of survival. In conclusion, every woman with operable breast cancer should be offered option of breast conservation if there are no standard contraindications. Even large tumors which do not allow for conservation initially can be downsized with prior chemotherapy. Surgeon′s education goes a long way in increasing rates of breast conservation. [30] References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11119f4.jpg] [cn11119f3.jpg] [cn11119f1.jpg] [cn11119t2a.jpg] [cn11119f5.jpg] [cn11119t1.jpg] [cn11119t2b.jpg] [cn11119f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}