 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
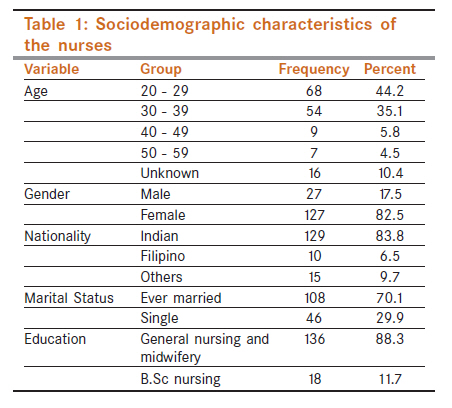
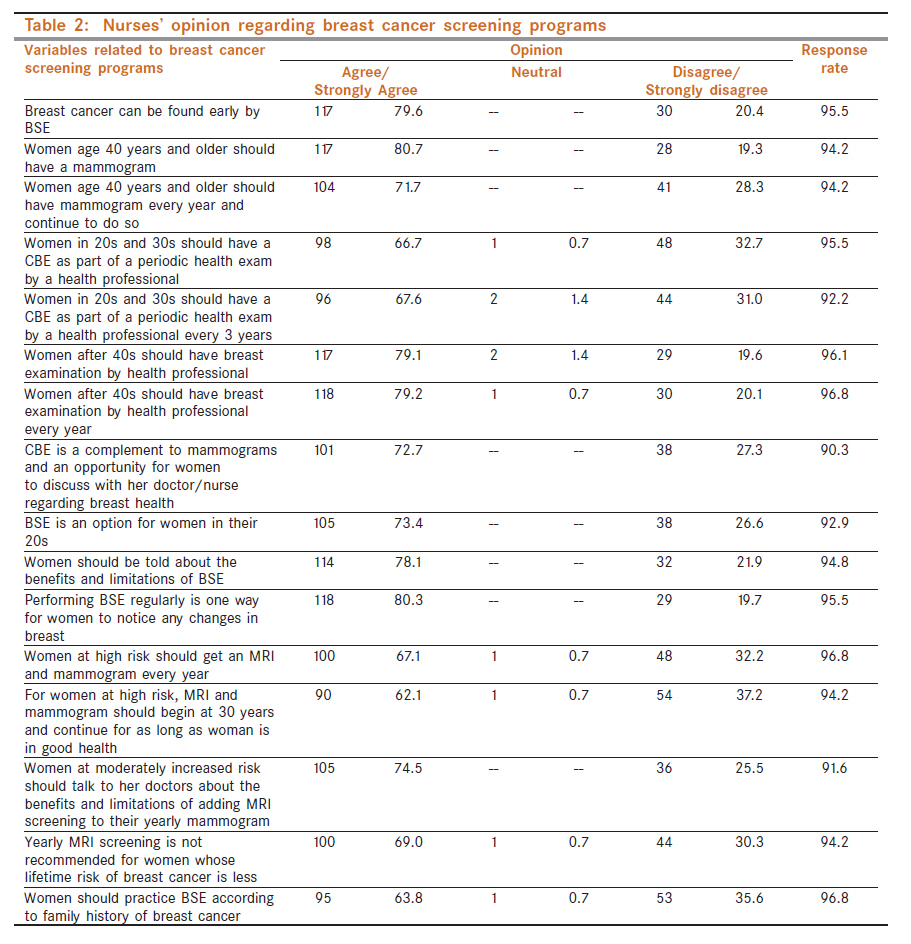
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 423-427 Breast - Original Article Opinion of nurses regarding breast cancer screening programs M Venkatramana1, J Sreedharan2, J Muttappallymyalil2, M Thomas1 1 GMC Hospital and Research Centre, Gulf Medical University, Ajman, United Arab Emirates Code Number: cn11120 PMID: 22293255 Abstract Aim: Found to be effective in its treatment. The increased incidence of breast cancer supports the implementation of breast cancer screening programs. The present study evaluates the opinion among nurses regarding breast cancer screening programs in United Arab Emirates (UAE). Keywords: Breast Cancer, breast screening programs, breast self examination, clinical breast examination, mammogram Introduction Breast cancer is the most common cancer seen in women worldwide. [1] Global incidence of breast cancer indicates an increase of 50-100% in the past 20 years.- [2] Breast cancer cases are estimated to have reached 1.2 million worldwide and globally every 3 minutes a woman is diagnosed with breast cancer amounting to 1 million new cases annually. [3] The incidence may possibly go up by 50% i.e., 1.5 million by 2020 as reported in the world cancer report 2008, also that breast cancer accounts for 16% of cancer deaths globally. [4] In the United Arab Emirates (UAE), breast cancer is among the top ten most common cancers occurring among the general population and is the second leading cause of death among women, accounting for 28% of all female deaths in 2005. [5] Early detection of breast cancer makes more treatment choices available and also there are greater chances of long-term survival. [6] Breast self-examination (BSE), clinical breast examination (CBE) and mammography are the methods for early breast cancer detection. Although BSE is considered as cost-free, simple, non-invasive intervention, [7] its benefit is controversial. [8],[9] However, both BSE and mammogram are effective measures to detect breast diseases. When detected at the early stage, breast cancer is curable, with a 100% survival rate for stage 0 and I. [10] It is also important for women to be aware of the importance of early screening. To develop breast cancer educational programs and prevention campaigns, it is crucial to comprehend nurse′s opinion regarding breast cancer screening programs. Health care providers, educational institutions and media are considered to be the important resources of dissemination of breast cancer knowledge to women. The nurses can play a pivotal role in educating women through specially designed learning programs in the health care setting, as well as, through community outreach approaches that suit the social and cultural setting. Nurses constitute a special group having characteristics most appropriate for disseminating information on breast cancer screening program to the women. Therefore we assessed the opinion regarding breast cancer screening programs among registered female nurses in a teaching hospital in Ajman, UAE. Based on the findings, relevant measures to improve knowledge of nurses could be implemented in the study area. Materials and Methods This cross-sectional study was conducted among nurses who are practicing in UAE. The current study was conducted among nurses practicing in UAE who attended the breast cancer awareness seminar organized in connection with breast cancer awareness week program in the year 2009. None of the nurses refused to participate. Ethics committee approval was sought before conducting the study and informed consent was obtained from the participants before administering the research instrument. In addition to sociodemographic characteristics, the questionnaire contained 20 items to collect information on perception of participants regarding breast cancer screening programs. The scale uses a 3-point Likert format with the coding strongly disagree and disagree (1), neutral (2), agree and strongly agree (3). The questionnaire comprised questions on perception of breast cancer, various breast cancer screening programs available and ideal time to undergo these screening programs. Perception: Operationally defined in this study as the participant′s beliefs of whether or not the performance of breast cancer screening programs are valuable health promotion activities and will lead to the identification of breast cancer, promote early diagnosis and treatment and thus attain greater survival rates. The questionnaire was reviewed by experts in the field for its face and content validity. The participants were asked to provide sociodemographic characteristics such as age, gender, education, marital status and to complete the questionnaire before the seminar. On the day of data collection, the questionnaire was distributed to the participants before the commencement of seminar. One investigator was available to clear any doubts related to the questionnaire and to collect the completed questionnaires from the participants. Data analysis was conducted with PASW 17.0 software (IBM, IL, Chicago). Descriptive statistics including means, standard deviations and percentages were used to describe knowledge and practice regarding BSE. χ2 test was used to compare percentages by sociodemographic characteristics. Pearson′s χ2 tests were used to examine the association between categorical variables. The significance level for all analyses was P≤0.05. Results Outline of the sociodemographic characteristics of the participants are depicted in [Table - 1]. The mean age was 31 years with a standard deviation of 7.3. The age of the participants ranged from 20 to 59 years. 79.1% of participants were married and the remaining were single. With regard to the nationality, majority (83.8%) were Indians. In the present study, 50% participants strongly agreed that performing BSE can detect breast cancer early, while 26% agreed that breast cancer can be detected by doing BSE, but 14.9% strongly disagreed with it and 4.5% of the respondents disagreed to this matter. Among the participants, 52.6% of the respondents strongly agreed that women aged 40 years and older should have a mammogram and 16.2% of the respondents strongly disagreed to this aspect. Thirty-nine percent strongly supported that women aged 40 years and above should have a mammogram every year and continue to do so, but 9.7% strongly disagreed to this. Among the respondents, 25.3% strongly agreed that women in their 20s and 30s should have a CBE as part of a periodic health examination by a health professional and only 5.2% strongly disagreed to this. The details are in [Table - 2]. Among the respondents, 28.6% strongly agreed that women in their 20s and 30s should have a CBE as part of periodic health examination by a health professional every three years and only 3.9% strongly disagreed to this. It was observed that, 41.6% of the respondents strongly agreed that after the age of 40 years, women should have a breast examination by a health professional but 8.4% strongly disagreed to this point. Among the respondents, 37.7% strongly agreed that women should have breast examination after 40 years by a health professional every year. 10.4% strongly disagreed and felt that there is no need for women after 40 years of age to have an annual breast examination by a health professional. More than 23.4% strongly agreed that CBE is a complement to mammogram and an opportunity for women and their doctor or nurse to discuss changes in the breasts, early detection testing and factors in the woman′s history that might make her more likely to have a breast cancer. 11.7% strongly disagreed. In the present study, 27.9% of the participants strongly agreed that BSE is an option for women right from age 20 onward. But 11% of the respondents strongly disagreed that BSE is an option for women starting in their 20s. About the benefits and limitations of BSE, 33.8% of the respondents strongly agreed that women should be told but 11.7% strongly disagreed with this. In the study, 42.2% strongly agreed that performing BSE regularly is one way for women to know how their breasts normally look and feel and to notice any changes, but 14.9% strongly disagreed to it. Twenty-six percent of the participants strongly agreed that women at a high risk of getting breast cancer should get an MRI and mammogram done every year. However, 9.7% of the participants disagreed to it. About 22% strongly agreed that women at high risk should begin screening with MRI and mammogram at the age of 30 years and continue as long as the woman is in good health. On the other hand, 7.1% strongly disagreed to this issue. About the benefits and limitations of adding MRI screening to their yearly mammogram 24% of the participants strongly agreed that women at moderately increased risk should be told however, this was strongly disagreed by 11% of the participants. Yearly MRI screening for women whose lifetime risk of breast cancer is less was strongly not recommended by 16.9%, but 3.2% strongly disagreed to this. More than 28% of the respondents strongly agreed that BSE should be performed according to the family history of breast cancer; however, 7.1% strongly disagreed to this aspect. Discussion The present study evaluated the perception of nurses with regard to breast cancer screening. Fifty percent of the respondents strongly agreed with the early detection of breast cancer by breast self examination (BSE). Reports by American Cancer Society suggest that women who perform BSE monthly are more likely to detect breast cancer in the early stages, thus influencing early treatment and hence yielding a better survival rate. [11] A study by Salem et al. concluded the need for breast cancer prevention and screening programs due to the increased frequency of breast cancer. [2] In a study by Agboola et al., 88.7% of the health care workers indicated breast cancer being common and may be detected early with BSE to im-prove chances of survival of the patients, 65.7% nurses opined starting BSE before 19 years of age. [12] In the present study, 27.9% nurses strongly agreed that women in their 20′s can optionally perform BSE. The present study indicated that 42.2% participants had the opinion that BSE helps women in understanding their breast changes. 33.8% nurses strongly supported the importance of providing information about the benefits and limitations of BSE to women. In a study by Dundar et al., only 23.4% participants reported health professionals as a source of information on breast cancer thus suggesting the enhancement of breast cancer awareness leading to an increase in the practice of screening programs. [13] In the present study, 28.6% respondents strongly recommended that BSE performance is based on the family history of breast cancer. Findings from the study by Montazari et al. indicated a significant relation between BSE to age, marital status, education, knowledge of breast cancer and screening programs but not to personal and family history of breast problems. [14] In this study, 52.6% of the study population strongly opined performing mammography among women aged 40 years and above and 39% respondents favored the suggestion that women aged 40 and above should have an annual mammogram regularly. The results of the present study is in accordance to the study by Nguyen et al. where one-third of the health care workers prescribed mammography as soon as their patients reached the age of 40 years, another one-third continued to do so after their patients reached the age of 69 years. [15] The results from the study by Rohlfs et al. demonstrated 32.7% women aged 30-49 years and 27.9% women aged 50-65 years as undergoing periodic mammography. The study also concluded age being an important sociodemographic variable associated with carrying out mammography. [16] Another study by Bare et al. indicated higher age group as the only factor that increased the probability of not undergoing mammography. [17] A study conducted by Lane et al. suggested CBE as an expected part of routine physical examination that is widely performed and is still recommended for breast cancer screening by many authorities such as American Cancer Society and reported approximately 5% of the cancers being missed by mammography. [18] In a study conducted by Spigel et al., 94% participants strongly agreed or agreed that CBE is important in the detection of breast cancer and almost all believed that it provided an important connection to the healthcare team. [19] In the present study, 23.4% nurses strongly agreed to CBE as a compliment to mammogram and considered it as an opportunity for women to discuss their breast health with the heath care worker. The current study also reported that 25.3% of the participants had the view that women in their 20′s and 30′s should have CBE as a part of their periodic health examination. A study by Nguyen et al. reported that a majority of the respondents believed in beginning CBE between 30 and 35 years of age. [15] In the present study majority of the participants opined performing MRI and mammogram for women at higher risk and to continue it as long as in good health. Majority of the participants also recommended informing women on the benefits and limitations of adding MRI screening to their yearly mammogram. Study by Saslow et al. recommended MRI screening for women with an approximately 20-25% or greater lifetime risk of breast cancer. [20] The guidelines from the American Cancer Society also stated that women with increased risk of breast cancer might benefit from the additional screening modalities such as MRI and ultrasound, beyond those offered to women at average risk like mammography and physical examination. [21] A study by Carney et al. suggested the need for closer surveillance by primary care clinicians for women at highest risk for breast cancer. [22] Another study by Edward et al. concluded that nursing practitioners can play an important role in cancer prevention by using appropriate tools to assess women′s breast cancer risk in primary care settings. [23] Conclusions The study signifies the need for implementation of workplace training programs for nurses, thus facilitating a better knowledge among them. The nurses should also be provided opportunities to disseminate their knowledge effectively among the general population leading to an increase in breast cancer awareness in the community. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11120t2.jpg] [cn11120t1.jpg] |
| |||||||||

{kind=link}
{kind=link}