 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
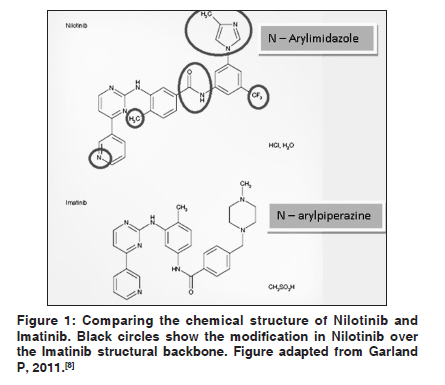
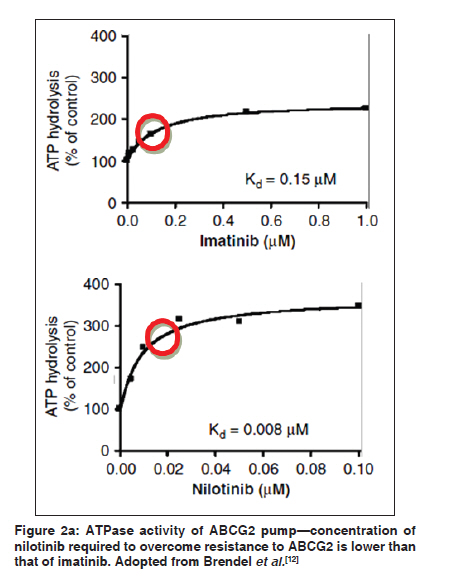
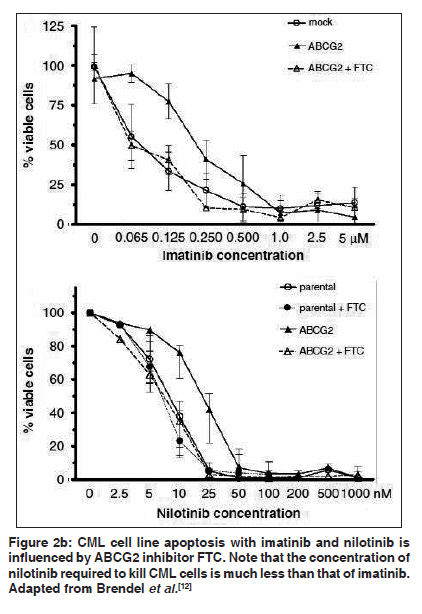
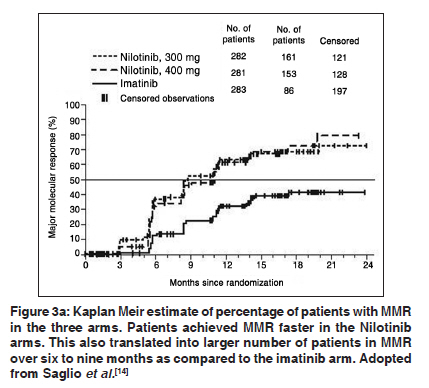
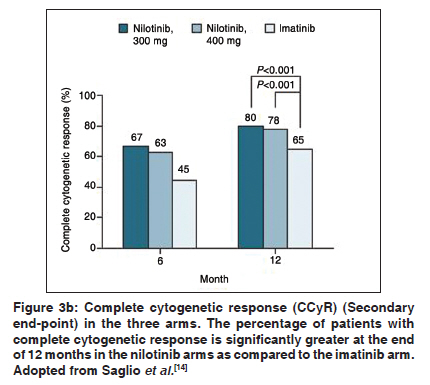
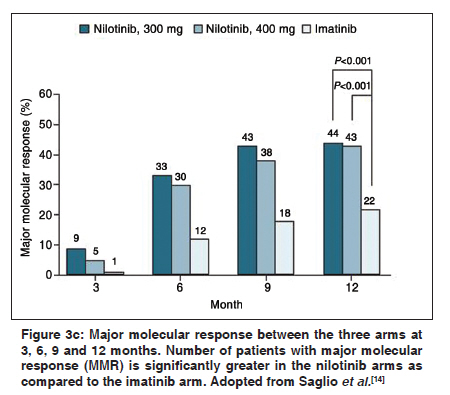
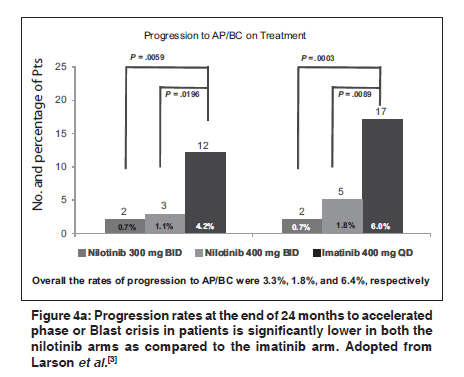
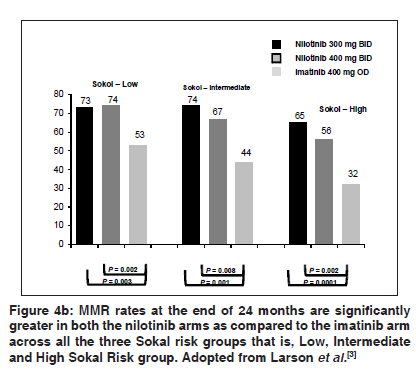
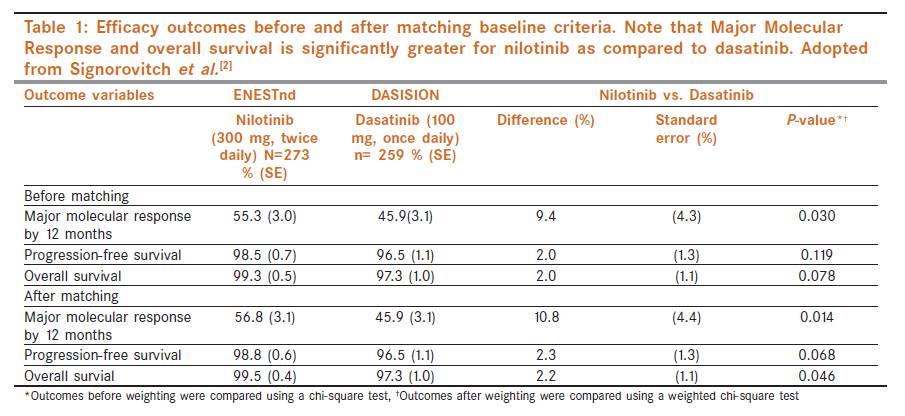
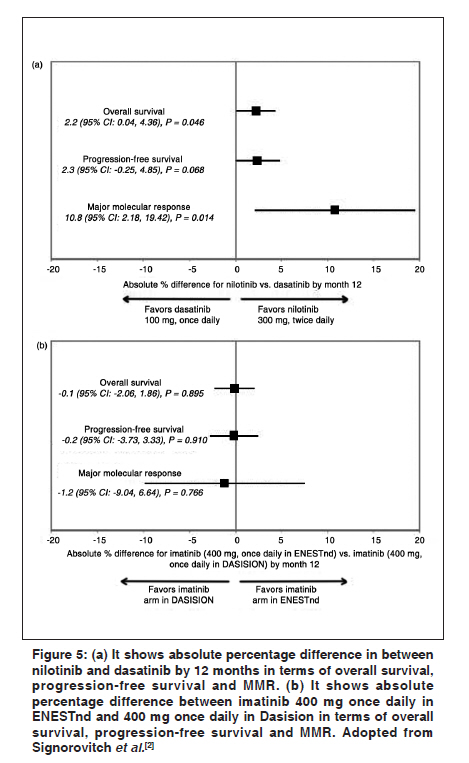
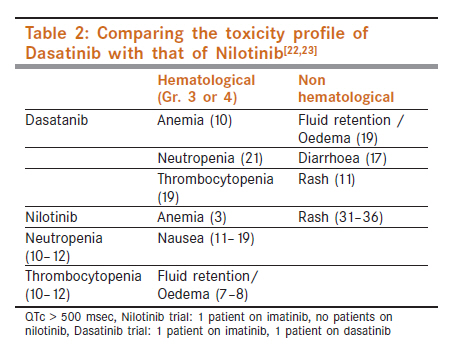
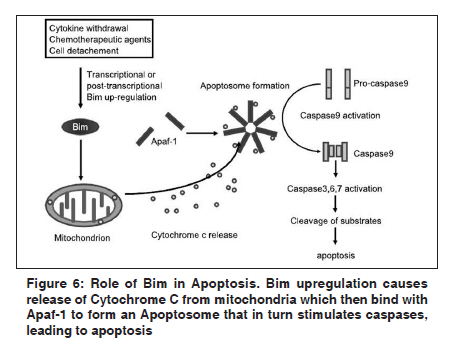
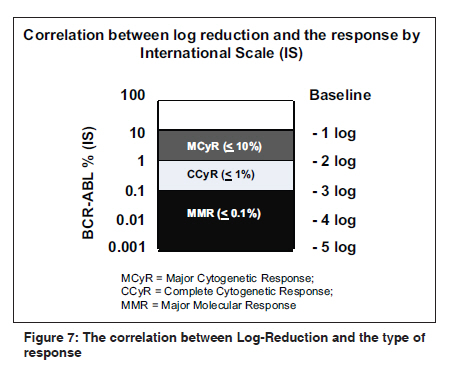
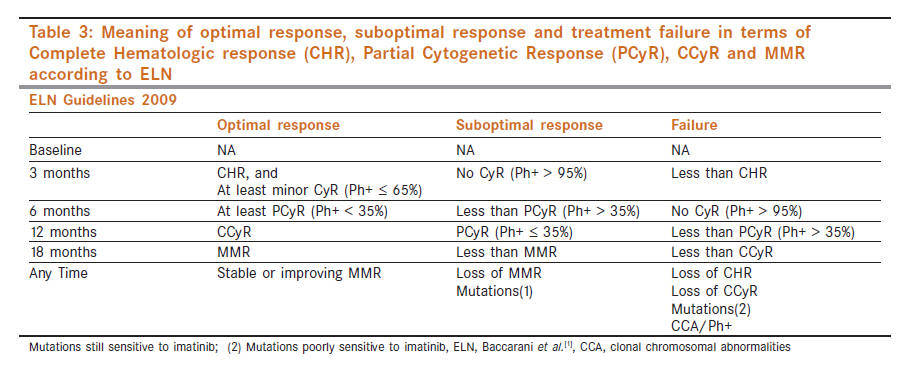
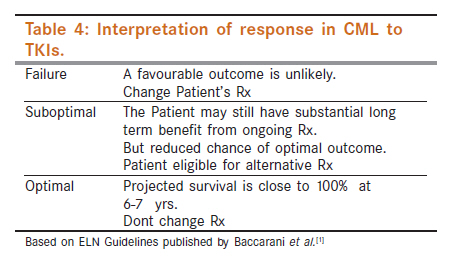
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 438-445 Hematological Malignancies - Review Article Nilotinib as first-line therapy for chronic myeloid leukemia A Vaid Department of Medical Oncology, Cancer Institute, Medanta Hospital, Medicity, Sector 38, Gurgaon, NCR, Delhi, India Code Number: cn11122 PMID: 22293257 Abstract Tyrosine Kinase Inhibitors brought a revolution in the management of chronic myeloid leukemia. Long term disease free survival became a reality for the majority of patients. With the identification of imatinib resistance and its implications, roles of newer targeted therapy molecules came into focus. Nilotinib data has matured and shows the fulfillment of earlier promise - even in first line therapy. This review provides insight into the place of this molecule in the first line management of chronic myeloid leukemia. Keywords: Tyrosine kinase inhibitor, response, safety, overcoming resistance Introduction Chronic myelogenous leukemia (CML) is a myeloproliferative disorder characterized by genomic instability and chimeric fusion gene as a result of balanced, reciprocal translocation between Chromosome 22 and Chromosome 9. The resultant BCR-ABL fusion protein has a constitutive tyrosine kinase activity that leads to uncontrolled proliferation of the myeloid cells. Prior to the imatinib era, the primary objective of CML therapy was to keep the white blood cell (WBC) counts under control and alleviate symptoms. Interferon allowed a small fraction of patients to even achieve significant cytogenetic response. However, it was only the systematic development of imatinib that led to a molecule capable of targeting the chimeric bcr-abl gene and preventing downstream effects of the tyrosine kinase activity. For the first time, a significant number of patients with CML were able to achieve complete hematological remission, disappearance of the Philadelphia clone and prolongation of life in the chronic phase. Unfortunately, the emergence of resistance, novel mutations and progression to Accelerated Phase and/ Blastic Crisis, forced us to search for more effective treatment options. Nilotinib - A second-generation tyrosine kinase inhibitor Nilotinib is an orally active, ATP-competitive, second-generation tyrosine kinase inhibitor (TKI) that selectively binds to the BCR-ABL protein. It also has activity against ABL, KIT and PDGFR-α and-β. It does not demonstrate direct activity against Src family kinases; however being downstream ABL kinase, it is subject to indirect inhibition. [4] Mechanism of action Nilotinib selectively and competitively binds to specific amino acid residues in BCR-ABL protein with 30 times more potency than imatinib. [5],[6] This binding on the phosphate-binding loop (p-loop) of the protein leads to protein folding over the ABL-ATP binding site and resultant blockage of the activation loop (a-loop) of the substrate binding site. Thus there is no catalytic activity of the BCR-ABL protein and its downstream targets are not triggered. [7] Nilotinib has also been shown to have pro-apoptotic properties through the promotion of bcl-2, thus acting like a tumor suppressor to leukemic cells (vide infra) [Figure - 1]. Nilotinib was designed specifically to mimic compounds binding to BCR-ABL mutants - using the imatinib structure as a backbone. Pharmacokinetics and pharmacodynamics Kantarjian et al., in 2006 [9] showed that Nilotinib takes 3 h to reach peak concentration following a single oral administration. It takes eight days to reach steady state concentration. Its elimination half-life is close to 17 h, with more than 90% of the drug being eliminated fecally and less than 5% in urine. [10] The majority of drug excretion is through the biliary route with only a small proportion being eliminated through gastrointestinal secretion. Nilotinib and human organic cation transporters Influx of imatinib into the cell depends on the expression level of human Organic Cation Transporters (hOCT) according to a study done by White et al. [11] This is because imatinib has the N-aryl piperazine group which connects to the hOCT on being protonated. On the other hand, nilotinib has the N-arylimidazole group which is weakly basic. Hence the intracellular uptake and retention for nilotinib is not transporter-dependent and is significantly greater-a significant pharmacokinetic advantage. This also explains why patients treated on imatinib with low hOCT levels are likely to have primary treatment failure [Figure - 2a and Figure - 2b]. [12] Nilotinib and ABCG2 ABC transporters such as MCR1 (ABCB1), MRP1 (ABCC1) and ABCG2 are also involved with TKI pharmacokinetics. Of these ABCG2 has been found by Brendel et al., to play a vital role in drug efflux of nilotinib. [12],[13] This also explains the hematological toxicity of all TKIs. ABCG2 present on normal progenitor cells (expression significantly less than on CML cells; present as a protective mechanism) is also inhibited by TKIs. Due to inhibition of normal hematopoietic progenitors by imatinib, nilotinib and dasatinib, some patients develop varying severity/ incidence of anemia, thrombocytopenia and neutropenia (myelosuppression). Advantages of nilotinib over lmatinib in CML remission Saglio et al., in 2010, [14] compared nilotinib with imatinib in a three-arm study with 300 mg nilotinib twice daily, 400 mg nilotinib twice daily and 400 mg imatinib twice daily. Primary and the secondary end-points of the study were major molecular response and complete cytogenetic response at the end of 12 months. Thus, nilotinib′s potency and selectivity for inhibition of BCR-ABL is better than that of imatinib. Further comparison between nilotinib and high-dose (800mg) imatinib finds that overall disease progression is higher in the imatinib arm as compared to nilotinib. Number of patients discontinuing therapy due to adverse events is also higher in the imatinib arm. [15],[16] A 24-month follow-up study of ENEST by Larson et al., [3] states that complete molecular response achieved with nilotinib is far greater than that with imatinib at 18 months with fewer deaths related to CML [Figure - 3a, Figure - 3b and Figure - 3c]. Also, this study effectively shows the number of patients with disease progression in all three arms. Refer to [Figure - 4a and Figure - 4b] for more details. In a similar analysis for molecular response with imatinib and nilotinib, the MMR rates were 46% for standard-dose imatinib, 54% with high-dose imatinib and 81% with nilotinib at 12 months. [17] GIMEMA and MDACC studies also confirm that patients on nilotinib have higher and faster achievement of MMR and CCyR. [18],[19],[20],[21] Thus all these studies clearly demonstrate that nilotinib is a faster and deeper-acting drug as compared to imatinib with lower risk of disease progression (to AP or BC). Thus, nilotinib at either dose is a much better drug than imatinib as first-line therapy in CML. Nilotinib compared to dasatinib for first-line therapy for CML: [22],[23] A study in 2011 indirectly compares the efficacy of nilotinib versus dasatinib in newly diagnosed CP-CML patients (a matching adjusted comparison) [Table - 1], [Figure - 5]. [2] It reported a significantly higher rate of MMR with nilotinib (56.8%) as compared to dasatinib (45.9%). It also reported higher rates of overall survival with nilotinib (99.5%) as compared to dasatinib (97.3%) at 12 months. Even the progression-free survival was found to show trends favoring nilotinib. This translated into better overall survival, 99.1% with nilotinib v/s 96.1% with dasatinib at a median time interval of 14 months. Moving on to comparing toxicities, myelosuppression is a common hematological adverse drug reaction with tyrosine kinase inhibitors. Among patients who demonstrated resistance or intolerance to imatinib therapy, the rates of Grade 3/4 neutropenia was 31% in chronic-phase and 42% in accelerated-phase CML patients on nilotinib therapy (dose - 400 mg twice a day) as compared to 36% in chronic-phase (dose - 100 mg once daily) and 58% in accelerated-phase (dose - 140 mg once daily) CML patients on dasatinib therapy. Grade 3/4 neutropenia was 12% in newly diagnosed CML patients on nilotinib therapy (dose - 300 mg twice a day) as compared to 22% in patients on dasatinib therapy (dose - 140 mg once daily). Similarly, Grade 3/4 thrombocytopenia was 30% in chronic-phase and 42% in accelerated-phase CML patients on nilotinib therapy (dose - 400 mg twice a day) as compared to 23% in chronic-phase (dose - 100 mg once daily) and 63% in accelerated-phase (dose - 140 mg once daily) CML patients on Dasatinib therapy. Grade 3/4 thrombocytopenia was 10% in newly diagnosed CML patients on nilotinib therapy (dose - 300 mg twice a day) as compared to 19% in patients on dasatinib therapy (dose - 140 mg once daily). This resulted in dasatinib-associated thrombocytopenia leading to serious central nervous system (CNS) hemorrhage (1%), gastro intestinal tract (GIT) hemorrhage (4%) and other severe (2%, unspecified locations) hemorrhages. Finally Grade 3/4 anemia was 11% in chronic-phase and 27% in accelerated-phase CML patients on nilotinib therapy (dose - 400 mg twice a day) as compared to 13% in chronic-phase (dose - 100 mg once daily) and 47% in accelerated-phase (dose - 140 mg once daily) CML patients on dasatinib therapy. Grade 3/4 anemia was 10% in newly diagnosed CML patients on nilotinib therapy (dose - 300 mg twice a day) as compared to 11% in patients on dasatinib therapy (dose - 140 mg once daily). Thus, myelosuppression associated with nilotinib therapy is much lesser as compared to that associated with dasatinib therapy. Even for non-hematological Adverse Drug Reactions, there is significant difference in the spectrum among TKIs. Dasatinib is associated with higher incidence of pleural effusions, severe pulmonary edema, and pericardial effusions. Pleural effusion was found to be 18% (all grades) in chronic phase (dose - 100 mg once daily) and 21% (Grade 3/4) in accelerated phase (dose - 140 mg once daily) in patients on dasatinib therapy. Whereas pericardial effusion was found to be 2% (all grades) in chronic phase (dose - 100 mg once daily) and <1% (Grade3/4) in accelerated phase (dose - 140 mg once daily). Fluid retention and diarrhea was also higher for dasatinib [Table - 2]. On the other hand nilotinib is associated with a higher incidence of nausea, rash and elevated amylase. Hence the toxicity profile of nilotinib is more favorable for almost all patients except for patients with known diabetes mellitus - where dasatinib may be safer. Role of Bcl-2 intermediate mediator protein in apoptosis and TKI therapy with Imatinib and Nilotinib It has been previously shown [24],[25] that Bim expression is downregulated in CML cells, thereby allowing evasion of apoptosis. Goodyear et al., [26] have also shown that lower levels of Bim also lead to expansion of cells and may play a role in progression to blast crisis. Thus Bim acts as a tumor suppressor. So now let us look at the pathway through which Bim causes apoptosis in a dysregulated cell. Nilotinib has been found to increase Bim expression thus shifting the equilibrium of dysregulated cell towards apoptosis. [27],[28] Monitoring CML patients while on therapy Monitoring CML patients on therapy is very important to check disease status at specific time points, efficacy of response and early signs of resistance. It is generally done by using quantitative PCR techniques such as real-time Polymerase Chain Reaction (RT-PCR) that looks at BCR-ABL transcript levels [Figure - 6]. [Figure - 7] defines Major Cytogenetic Response (MCyR), Complete Cytogenetic Response (CCyR) and Major Molecular Response (MMR) in terms of percentage of BCR-ABL transcript level attained. Thus, MCyR is achieved at -2 log reductions, CCyR at -3 log reductions and MMR at -5 log reductions. Patients are monitored for therapeutic response at 3, 12 and 18 months [Table - 3]. At these time intervals optimal response, suboptimal response and therapeutic failure is defined in terms of the below mentioned end points. [Table - 4] explains the interpretation of optimal response, suboptimal response and therapeutic failure and steps to be taken. To summarize, if there is an optimal therapeutic response then there is no need to change therapy. If the patient has suboptimal response then the patient may not have 100% survival or longer progression-free survival and patient is eligible for an alternative drug that may give better response. However, if the patient has therapeutic failure then it is advised to change patient′s therapy. Precautions to be taken when using nilotinib for CML [22] Concomitant administration with food increases nilotinib drug-blood levels. Since this effect is variable, blood levels are also elevated in a highly variable manner. Hence no food should be taken 2 h before and 1 h after administration of nilotinib. Nilotinib prolongs the QT interval and hence is contraindicated in patients with pre-existing prolonged QT interval syndromes. Hypokalemia and hypomagnesemia also prolong the QT interval and hence these conditions should be corrected before starting the patient on nilotinib. Concomitant use with strong CYP3A4 inhibitors such as ketoconazole, rifampin, etc., antiarrhythmics such as quinidine, and drugs that prolong the QT interval such as cisapride, dofetilide, dronedarone etc., should be avoided; if concomitant use is clinically warranted, dosage adjustment and monitoring is recommended. Similarly concomitant use with grapefruit products should be avoided as it reduces the blood levels of nilotinib. For patients who have undergone total gastrectomy, nilotinib blood levels are reduced. Hence more frequent monitoring, appropriate increase in dosage or alternative treatment may be necessary. If patient shows hepatic impairment standard nilotinib dose may lead to delayed clearance and higher blood levels. Thus lower than normal initiating doses as well as monitoring at regular intervals may be warranted. Nilotinib may also precipitate liver toxicity such as elevated bilirubin, AST/ALT, and alkaline phosphatase levels. For patients with history of pancreatitis, nilotinib use may increase serum lipase levels and thus monitoring is recommended. Finally, it is important to keep in mind that the safety of nilotinib has not been evaluated in the presence of pregnancy. Since imatinib has been found to be generally safe in such situations, serious problems are not anticipated. Is there a role for combining Nilotinib with other TKIs? Nilotinib in not effective against all phases of the cell cycle, for example, cells in G0 phase would remain unaffected. [29],[30] Cells with activated Lyn kinase (Src family), a gene involved downstream to BCR-ABL, could also remain resistant to nilotinib. [13],[31] A combination of nilotinib and dasatinib thus has the potential to benefit selected patients by synergistic action (dasatinib is a Src inhibitor and hence the mechanism of action is partially non-overlapping). [31] Unfortunately, combining nilotinib and dasatinib might still leave the most primitive dormant stem cells unaffected and hence the risk of relapse and resistance is not totally eliminated. [30],[32] Conclusion Management of CML is a landmark success story in the era of targeted and personalized therapy. The first oral TKI, imatinib, brought a revolution in the approach to the management of this disease - relegating transplantation to second line. With the identification of resistance to imatinib, the quest was on to find alternate molecules, the second-generation TKIs. Both dasatanib and nilotinib are active in patients resistant or intolerant to imatinib. Subsequent studies showed that they are also active in first-line setting - with the advantage of faster, deeper and longer response. Amongst these two, nilotinib is found to be the safer, better tolerated and more efficacious drug and is a clear choice in most patients newly diagnosed to have chronic-phase CML. Preliminary studies indicate that, in the future, efficacy may be improved further by combining nilotinib with other cytokine inhibitor that induces Bim (pro-apoptotic and a G0 poison for dormant primitive CML cell) in a synergistic manner. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11122f5.jpg] [cn11122f4a.jpg] [cn11122f1.jpg] [cn11122t3.jpg] [cn11122f2a.jpg] [cn11122f7.jpg] [cn11122f4b.jpg] [cn11122t2.jpg] [cn11122t1.jpg] [cn11122f2b.jpg] [cn11122f3b.jpg] [cn11122f3c.jpg] [cn11122f3a.jpg] [cn11122t4.jpg] [cn11122f6.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}