 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
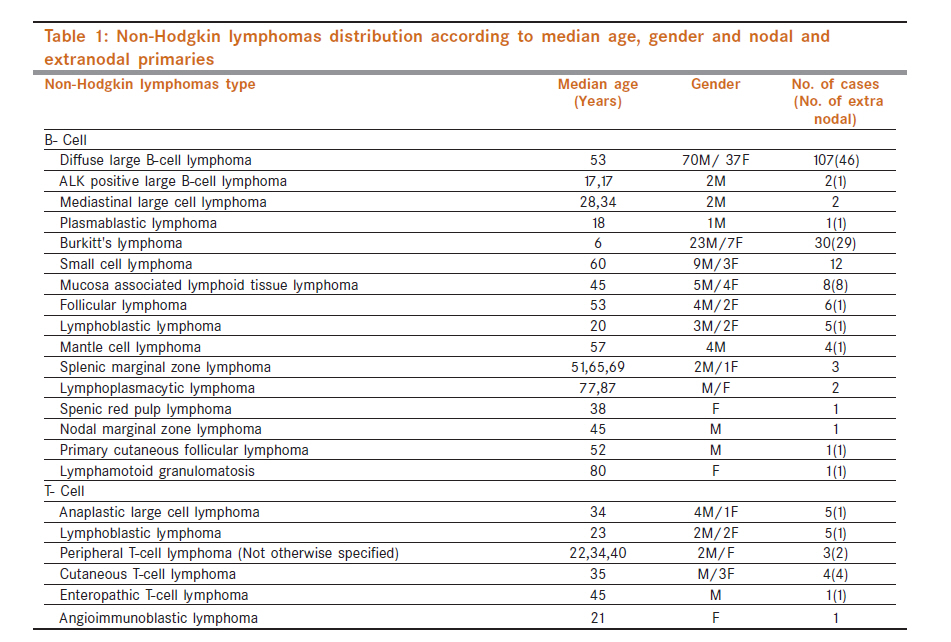
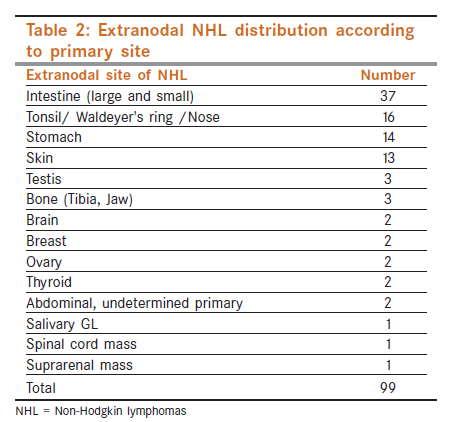
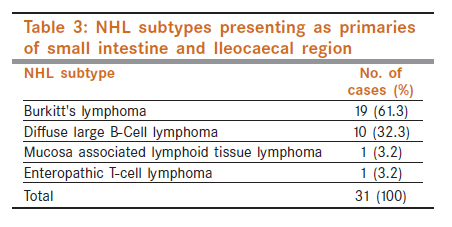
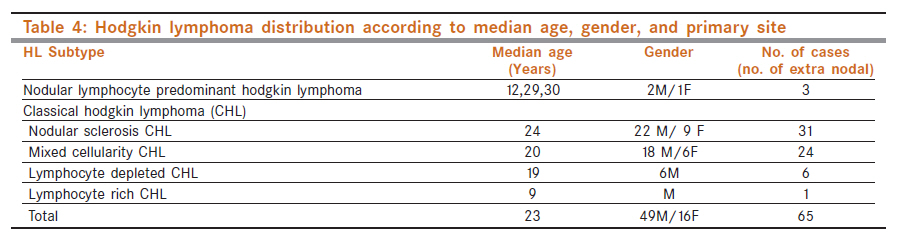
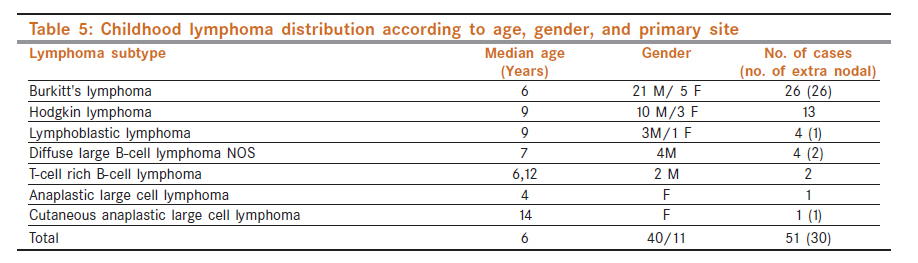
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 446-451 Hematological Malignancies - Original Article Malignant lymphoma in northern Iraq: A retrospective analysis of 270 cases according to the World Health Organization classification RT Yaqo1, MD Hughson2, FK Sulayvani3, NA Al-Allawi1 1 Department of Pathology, College of Medicine, University of Dohuk, Iraq Code Number: cn11123 PMID: 22293258 Abstract Background: Based on the World Health Organization (WHO) classification, the distribution of various subtypes of malignant lymphoma (ML) appears to differ by geographical region. Keywords: Iraq, immunophenotyping, lymphoma, World Health Organization classification Introduction Since its introduction in 2001, the World Health Organization (WHO) classification of malignant lymphoma (ML) has gained popularity and has been applied to the classification of these malignancies in various populations around the world. [1] Studies from Western Europe, North America, Japan, China, India, and some Middle Eastern countries have revealed that the relative proportions of various ML as determined by this classification differs with geographical region. [1],[2],[3],[4],[5],[6],[7],[8] ML is the third most common reported malignancy in Iraq, [9] but there are few published Iraqi studies on the subject [10],[11],[12],[13],[14] and none have addressed the relative distribution of the various subtypes based upon the WHO classification. This study was undertaken in order to determine the types of ML occurring in the country as based upon the WHO updated classification [15],[16] and to compare the distribution of diagnoses with published studies from nearby Middle Eastern countries as well as other developed and underdeveloped regions of the world. Materials and Methods The study material consists of Malignant Lymphomas diagnosed by the two main referral laboratories in Northern Iraqi provinces of Dohuk and Sulaimania in the period between June 2003 and February 2010. These Laboratories serve a population of around 3 millions of mainly ethnic Kurds, which are the second largest ethnic group in Iraq (following Arabs) and live mainly in its northern region. The material was subjected to a retrospective independent pathological review by the three pathologists involved in this study (RTY, MDH, and NAA). The records of all patients were also reviewed particularly in relevance to age, sex, and primary site of involvement. Plasma cell dyscrasias and leukemias were excluded from this study. Lymphomas were categorized as primary extra nodal, if they arose from tissues other than lymph nodes, spleen, or thymus. [17] Sections from paraffin-embedded tissue blocks were prepared and used for standard Hematoxylin and Eosin (H and E) stain and for immunohistochemical staining using the streptavidin-biotin peroxidase method. The antigens were unmasked by heat induced epitope retrieval using citrate (pH 6.1) or Tris-EDTA (pH 9) buffers as recommended for individual antibodies. Heat was applied by a steamer for 40 minutes. The panel of antibodies consisted of: CD3, CD4, CD5, CD8, CD10, CD15, CD20, CD23, CD30, BCL2, BCL6, CD79a, anaplastic lymphoma kinase-1 (ALK-1), Cyclin D1, Terminal deoxynucleotidyl Transferase, and Ki67 (Dako, Denmark). The reviewers prepared further H and E slides and/or additional immunohistochemistry whenever appropriate. Based on morphology, appropriate immunohistochemistry results and the consensus opinion of any two of the three pathologists involved, cases were diagnosed as Hodgkin lymphoma (HL) or a specific category of Non-Hodgkin lymphoma (NHL) according to the WHO updated classification. [15],[16] This study was conducted in compliance with the Helsinki accords and was approved by the ethical committee at the college of Medicine, University of Dohuk, Iraq. Results There were 270 ML included in the study. NHL was diagnosed in 205 (76%) and HL in 65 cases (24%). Non-Hodgkin lymphoma The age range of NHL patients was 2−87 years with a median age of 45 years. They included 137 males and 68 females (male to female ratio 2:1). [Table - 1] outlines the categories of NHL classified according to 2008 WHO scheme and it shows B-cell phenotypes in 91% and T-cell in the remaining 9%. Diffuse large B-cell lymphoma (DLBCL) was the most common diagnosis at 52.2%. Among diffuse large B-cell lymphoma, DLBCL (Not otherwise specified) was the most frequent (48.8% of NHL) followed by T-cell rich B-cell lymphoma (TCRL) at 2.9% and primary CNS DLBCL (1%). The second most common NHL was Burkitt′s lymphoma (BL) seen in thirty patients (14.6%), followed by Small lymphocytic lymphoma in 12 cases (5.9%) and Mucosa associated lymphoid tissue (MALT) lymphoma in 8 cases (3.9%). Follicular lymphomas were only diagnosed in 6 cases (2.9%), while B-Lymphoblastic lymphoma, Mantle cell lymphoma and splenic marginal zone lymphoma were less frequent. Other B-cell Lymphomas are outlined in [Table - 1]. Of T-cell lymphoma, anaplastic large cell lymphoma, T-Lymphoblastic lymphoma, peripheral T- cell lymphoma (NOS) were the most frequent at 2.4%, 2.4%, and 1.5% of NHL respectively. Four patients had cutaneous T-cell lymphomas, two with mycosis fungoides (both females aged 45 and 50 years) and two with cutaenous CD30 positive anaplastic large cell lymphoma (one male and one female aged 14 and 25 respectively). One hundred and six NHL (51.7%) were nodal primaries and presented with cervical, axillary, or inguinal lymphadenopathy in 60 patients, 25 had lymphadenopathy involving two or more of these regions, 11 with splenic primary, four patients presented with abdominal lymphadenopathy, three with mediastinal lymphadenopathy, and three with non-specified nodal primaries. Primary extra nodal NHL were found in 99 patients (48.3%), with the intestine being the most frequent site in 37 cases, followed by the Waldeyer′s ring, stomach, and skin [Table - 2]. All 8 MALT lymphomas, 29 of 30 (96.7%) Burkitt′s lymphomas and 46 of 107 (42.9%) DLBCL were extra nodal. The latter two NHL subtypes constituted the bulk of primaries involving the small intestine and Ileocaecal region [Table - 3]. Hodgkin lymphoma The age range of HL patients was 2.6−76 years with a median age of 23 years. There were 49 males and 16 females (male to female ratio 3:1). Of the 65 patients with HL, 31 had nodular sclerosis (NS) (48 %), 24 had mixed cellularity (MC) (37 %), 6 were lymphocyte depleted HL (9.2 %), three had nodular lymphocyte predominant HL (4.8%) and one had lymphocyte rich HL (1.5 %). [Table - 4] outlines the age and gender distribution of HL cases according to subtype. All cases of HL presented with nodal primaries. The primary biopsies sampled were most frequently cervical lymph nodes in 40 patients (61.5 %), followed by the axillary, abdominal, anterior mediastinal and inguinal in 9.2, 7.7, 3.1 and 1.5% of cases respectively. While eight cases (12.3%) involved multiple nodal groups, and the remaining three were of non specified nodal primary. Lymphoma in children The study included 51 children who were defined as individuals 15 years old or less. Twenty-six (51%) were diagnosed as BL, 13 (25.4%) as HL, four as DLBCL (7.8%). Of the remaining eight patients: four children had precursor LBL (2 TLBL and 2 BLBL), two cases of T-cell rich large B-Cell lymphoma, and one case each of cutaneous large cell lymphoma and CD30 positive anaplastic large cell lymphoma, the latter with retroperitoneal lymphadenopathy with hepatosplenomegally. [Table - 5] summarizes the clinical and pathologic features of the childhood lymphomas. All the 26 BL cases were extra nodal primaries. The intestine was the primary extra nodal site in 21 patients while the maxillary bone was the site in only one patient. The remaining four extranodal cases involved the Waldeyer′s ring. Of the latter, two cases involved the pharyngeal tonsil and two presented as nasopharyngeal masses. Discussion The importance of the current study is that it documents the relative distribution of various types of lymphoma in a geographical area that has not been previously investigated. With other similar studies from the Middle East, it is hoped that it will contribute toward a better understanding of potential predisposing factors for ML in this part of the world. Among the patients in this study, one HL has been diagnosed for every three NHL. This rate of 31 % is similar to the 30% seen in west [1] and appears to be within the range reported from surrounding Eastern Mediterranean countries as well as India where rates varied from 21.6% in Jordan to 41% in UAE. [18],[19],[20],[21],[22],[23],[24] These findings contrast with the much lower frequency in East Asian countries such as Japan where HL constitutes only 7% of ML in a recent large study. [4] The most frequent histological subtype of HL in the current study was NS, which is different from earlier reports from Iraq, [10],[11] and some earlier reports from nearby countries and India, [6],[19],[22],[23],[24],[25] in which the mixed cellularity subtype was the most frequent. This changing pattern is consistent with more recent reports from Saudi Arabia, Jordan, UAE and Kuwait, where higher relative rates of NS HL were reported approaching those seen in the United States and Europe. [1],[15],[7],[18],[21],[26] Al-Diab et al from Saudi Arabia suggested that this trend may be related to urbanization and improvement in the living standards. [7] This may have led to a reduced risk of early childhood exposure to Epstein Barr virus that is more likely to be associated with MC rather than NS HL. [7] We found that DLBCL was the most frequently encountered NHL accounting for 52.2% of these diagnoses. DLBCL has also been reported to be the most common NHL in most studies worldwide, but it varies considerably from region to region. The relative proportion of DLBCL in the current study is almost twice the 25−30% seen in the USA and Europe and is much higher than the 33−37% reported in India [1],[3],[15],[27],[28] but is closer to figures reported UAE at 59%, [21] Kuwait 47.6%, [29] Egypt 49%, [8] Jordan 43.8%-53%, [18],[30] and Turkey at 41%. [31] Moreover, 44.9% of DLBCL presented with extra nodal disease, and a majority of the extra nodal primaries were gastrointestinal. This is a pattern that has been reported worldwide. [1],[15] In contrast to the high rates of DLBCL, FL was found to account for less than 3% of our NHL. This is in marked contrast to the 28−32% of NHL in Western studies [3] and is much lower than the 13−15% reported from India, [27],[28] but resembles rates in many nearby Mid-Eastern countries, where figures of 5%−8.1% were reported from Egypt, Saudi Arabia, Southeast Turkey, UAE, and North Jordan. [8],[21],[30],[31],[32] Figures of 3.8% and 3% were also reported from the Asian countries of Thailand and Pakistan, respectively. [8],[33] Such geographical variation in FL has long been recognized, and it has been suggested that there are different molecular pathways in ML development in different geographical areas. [34] The latter was inferred by the significantly lower incidence of bcl2 gene rearrangements, the hallmark of FL, in Asian compared to Western countries. [34] Naresh et al. proposed that the low rates of FL compared to DLBCL in developing countries may be the result of many DLBCL having progressed from previously undiagnosed FL, and that unique regional genetic or environmental factors may have contributed to such progression. [8] Nevertheless, this explanation would not seem to apply to nearly half of DLBCL which were extra nodal, since FL is predominantly nodal in origin. [1] It is possible that some of the extra nodal abdominal DLBCL were prior undiagnosed MALT lymphomas in which tumors had undergone a large cell transformation. Small Lymphocytic Lymphoma (SLL) was identified in 5.9% of our patients, which is comparable to Western reports at 7-11% [3],[35] and to rates reported from Jordan, Egypt, Kuwait, and India at 3.7−6%. [8],[27],[18] Similarly, MALT lymphoma was found in 3.9% of our patients, which is similar to reports from Egypt, Kuwait, UAE, Jordan and India at 2-4% [8],[27],[18],[21] and some Western countries at 3−7%. [3] MCL was diagnosed in four patients (2%), which may be somewhat lower than is seen in Egypt (4%), Jordan (6.2%), India (3.0−5.1%), [8],[27],[28],[18] and in Western countries (7%). [3] The current study and similar reports from some of the surrounding Middle East countries as well as the West show a low relative proportion of T-cell lymphomas. [2],[8],[21],[22],[30],[31],[35] This is in contrast to its high proportion in Far Eastern countries like Japan, China, and Korea were it constitutes 27−30.5% of NHL, [4],[5],[36] and to a lesser extent the 15-18% reported from India. [27],[28] Such significant variation in the geographical distribution of T-cell lymphomas has long been recognized and has been attributed to racial predisposition, HTLV-I viral infection and lower relative incidence of B-cell NHL in the Far East. [1],[3] In the current study, the second most common NHL, and the most common NHL in children was BL. Such predominance of BL is similar to earlier studies from Iraq [14] and to recent studies from Jordan, Saudi Arabia, and the UAE, [8],[18],[21],[30] but is different from Indian reports where BL ranks only third in frequency among children following precursor T-lymphoblastic lymphoma and DLBCL. [37] Twenty one of our 26 children with BL presented with intestinal primaries. In a 1979 Iraqi study by Al-Attar et al., primary abdominal tumors were documented in 90% of BL patients. [12] The abdominal presentation is seen in sporadic or non-endemic form of the disease throughout the world, except that outside the Middle East the frequencies of BL do not exceed 5% of NHL, and in most countries are in the range of 1−3%. [9],[15],[28] Such high relative frequency of BL in the populations of the Eastern Mediterranean requires further scrutiny, and is currently the subject of an ongoing study by our group. The current study on Iraqis describes a large proportion of extra nodal NHL lymphoma (48.3%) that is comparable to the rates observed in Kuwait (54%), [29] Southeast Turkey (44.5%), [31] and Jordan 40.8%, [30] but contrasts with the much lower figure of 26% found in North America. [38] The most frequent primary extra nodal sites were gastrointestinal tract, Waldeyer′s ring and skin, which are the usual extra nodal sites reported worldwide for NHL. [39] However, unlike most Western studies, but similar to some from the Middle East, the intestinal far outnumbered the gastric primaries. [13],[17],[31] The latter is partly due to large numbers of intestinal BLs in our series. However, and in contrast to earlier studies from central Iraq and some other Middle Eastern countries, [13],[40] no cases of Immunoproliferative small intestinal disease (IPSID) were documented in the current study. The latter observation is interesting and maybe due to late presentation with IPSID already transforming to Large B-Cell Lymphoma at diagnosis (more than one third of small intestinal cases were DLBCL), or it maybe related to the fact, that the current study was conducted in northern Iraq where the population is predominantly of the Kurdish ethnic group unlike that of central Iraq and other Middle Eastern countries where they are mostly Arabs. Another explanation may lie in the observation reported by several studies suggesting a decline in the incidence of IPSID in the Middle East over the past three decades, in fact one recent study from nearby Jordan also failed to find any cases of IPSID. [30],[40] Conclusion Our results show that among NHL, there is a high frequency of DLBCL and extra nodal primaries coupled with a low frequency of FL. Childhood abdominal BL was the second most common NHL. These findings are in marked contrast to the West but are similar to many countries in the Middle East. Further investigation of these differences will require a registry of regional lymphomas within a formal database and an estimate of the age specific incidence of the different diagnostic categories. HL comprised one third of ML diagnosed in our region, and in contrast to earlier studies, an emerging trend was observed whereby NSHL surpassed the MCHL as the most frequent HL, which is similar to the trend in some other Middle East countries and approaching the pattern seen in western countries. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11123t5.jpg] [cn11123t1.jpg] [cn11123t3.jpg] [cn11123t2.jpg] [cn11123t4.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}