 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
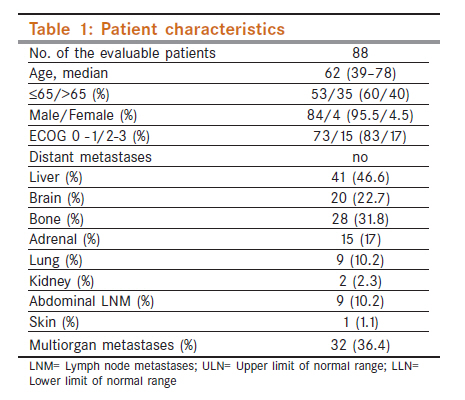
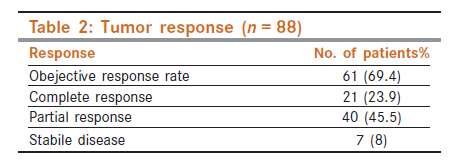
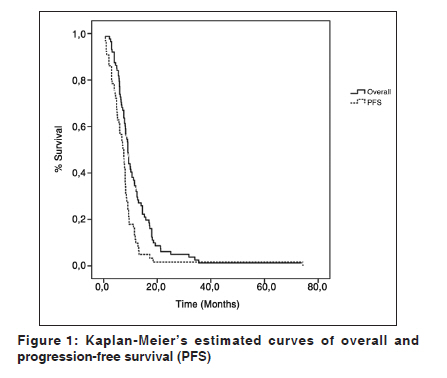
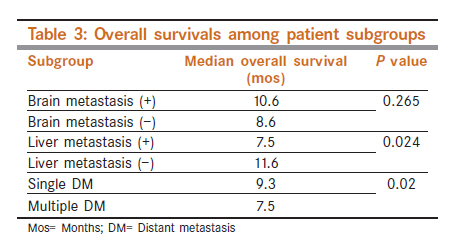
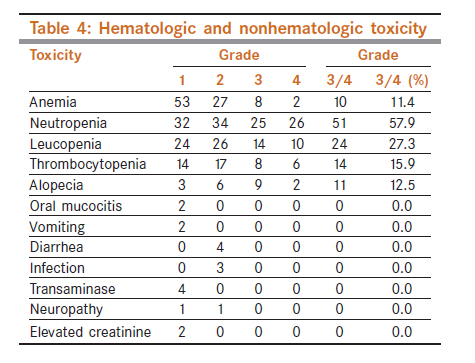
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 454-459 Lung - Original Article Carboplatin plus etoposide for extensive stage small-cell lung cancer: An experience with AUC 6 doses of carboplatin U Yilmaz, G Polat, C Anar, H Halilcolar Department of Pulmonary Medicine, Suat Seren Chest Disease and Surgery Training and Research Hospital, Izmir, Turkey Code Number: cn11125 PMID: 22293260 Abstract Aims: The aim of this study is to investigate the activity and toxicity of etoposide with AUC 6 doses of carboplatin in patients with previously untreated extensive disease - small-cell lung cancer (SCLC). Keywords: Carboplatin, chemotherapy, etoposide, metastatic disease, platinum Introduction In the Turkey, approximately 5 000 people are diagnosed with small-cell lung cancer (SCLC) each year, representing approximately 15.4% of all lung cancer cases. [1] The majority of these patients are diagnosed with extensive-stage disease (ED). One of the frequently used combination chemotherapy regimen for SCLC is cisplatin (P) and etoposide (E). [2] At the time this study was designed, the systematic review published by European Lung Cancer Working Party (ELCWP), comprising of a total 36 trials, demonstrated a survival benefit in favor of chemotherapy regimens including etoposide alone or in combination with cisplatin. [3] In another meta-analysis, patients receiving a cisplatin regimen proved to have a better probability of being responders, and a better survival than a regimen without this alkylating agent. [4] Cisplatin yields a putatively high toxicity (mainly nephrotoxicity, ototoxicity, and emesis). This can be problematic in the more fragile and elderly patients or in patients with cardiac or renal comorbidity. Carboplatin, an active analoque of cisplatin, has the advantages of easier administration, and less gastrointestinal, renal, auditive, and neurologic toxicities. Its hematological toxicity remains limiting, particularly in elderly patients. [5],[6],[7] The replacement of cisplatin by carboplatin (C) in the PE combination showed an identical complete response rate, comparable median survival, and less toxicity in the randomized trials. [8],[9],[ 10] But, when current trial was designed in 2000, the efficacy of carboplatin plus etoposide regimen had not been evaluated sufficiently. Thereafter, some authors reported that this substitution does not appear to be justified in everyday practice until results of confirmatory randomized studies clearly demonstrate whether the activity of these two platinum compounds is really similar. [11],[12] The carboplatin AUC is well predicted by the Calvert formula, based upon individual renal function, and correlates well with toxicity and tumor response in ovarian cancer. [13] Increasing carboplatin AUC above 5 to 7 mg/ml x minutes does not improve the likelihood of response but does increase myelotoxicity. Etoposide has been administered in a variety of doses and schedules. Etoposide doses per cycle have been varied widely from 180 to 510 mg/m2 (variation from 60 to 165 mg/m2 on days 1-3 of treatment cycles). Although increasing the etoposide dose per cycle has resulted in increased complete response rate, the overall response rate and survival have not been affected by dose variations. [14] Okamoto et al. performed a phase II study to determine the efficacy of carboplatin, dosed to a target AUC of 5 plus etoposide for elderly patients with SCLC. [15] They concluded that AUC-based carboplatin and etopside is an active and relatively nontoxic regimen in elderly patients. When current trial was designed in 2000, the efficacy and tolerability of the combination of carboplatin (AUC 6) on day 1 with intravenous etoposide 100 mg/m 2 on days 1 to 3 were unknown clearly. The purpose of the present study was to assess the efficacy of this regimen in patients with previously untreated ED-SCLC. Materials and Methods This is a retrospective cohort study using prospective database. Patients with histologically or cytologically proven ED-SCLC, including no prior thoracic radio or chemotherapy, ECOG performance status 3 or better, age ≥18 years were eligible. Patients were required to have adequate hematological (White blood cell count >3 000/μl, absolute neutrophil count ≥2 000/μl, hemoglobin level ≥10 g/dl, platelet count ≥100 000/ μl), hepatic (bilurubine ≤1.5 mg/dl, AST ≤2.5 x the upper limit of normal (ULN) or ≤5 x ULN if liver metastases were present), and renal functions (creatinine concentration ≤1.5 mg/dl, blood urea nitrogen ≤1.5 times normal). Patients were not eligible for the study if they had experienced any of the following events: Active infection, pregnancy or lactation, hypersensitivity to the study drugs, and concomitant or previous malignancies (except for adequately treated basal or squamous cell carcinoma of skin, carcinoma in situ of the cervix, or localized low-grade prostate cancer). The protocol was approved by the institutional review board. Each patient provided written informed consent. Pretreatment evaluation consisted of medical history, physical examination, complete blood count, biochemical screen, electrocardiogram, chest X-ray, CT of the chest, brain, and upper abdomen (or ultrasounography), and bone scintigraphy. The distinction between limited and extensive disease was made as follows: Limited disease (LD) was defined as disease restricted to one hemithorax with regional lymph node metastases, including hilar, mediastinal, and supraclavicular nodes, whether ipsilateral or contralateral. Patients with pleural effusion (cytologically positive or negative) were included in LD category. [16] ED was defined as disease beyond that included above. Patients were generally treated as outpatients. The regimen consisted of IV carboplatin AUC 6 (using the Calvert formula) on day 1 with IV etoposide 100 mg/ m 2 on days 1 through 3. Chemotherapy was repeated every 3 weeks for a maximum of six cycles. Treatment was delayed for up to 36 days to allow neutrophil levels to return to ≥2 000/μl, platelet levels to return to ≥100 000/μl. For grade 3 to 4 nonhematologic toxicities, treatment was delayed until resolution. If the hemoglobin level was less than 10.0 g/dl, blood transfusion was made. In patients with neutropenic fever and with more than 10 days of neutropenia, the doses of carboplatin and etoposide were adjusted to 75% in subsequent courses. Granulocyt colony-stimulating factor (G-CSF) was given only in patients with febrile neutropenia. The use of erythropoietin was not allowed owing to local policy. Before each cycle, the following assessments were made: Medical history, physical examination, blood chemistry, blood count, chest x-ray graphy, electrocardiogram, performance status, and clinical tumor assessment. Complete blood count was made on day 8 or 10 to define toxicity. Response assessments were performed, with repeat of CT chest scan and other abnormal investigation, after fourth and sixth cycles of chemotherapy. Besides, patients were assesable for response if they had received at least one full treatment course, and revisited to our hospital in the second treatment course. Tumor responses were assessed according to the World Health Organization (WHO) criteria. Patients were assessed for toxicity before each cycle according to WHO-Common Toxicity Criteria. The primary aim of the study was overall survival (OS). Secondary aims were progression-free survival (PFS), response rate, and toxicity. OS time was calculated from the first day of treatment until death or last contact. PFS was measured from the first day of treatment until the date of first progression or death without documented disease progression. Patients alive without progression were censored at the last time known to be in remission or stable. Survival curves were estimated by the method of Kaplan-Meier. Ranges, 95% confidence interval (CI) on the treatment estimates were computed. The cut-off date for the survival analysis was April 2010. Statistical analyses were performed using the SPSS version 10.0 statistical software. Results Between January 2001 and July 2009, there were 92 patients who met the eligibility criteria for this study. Of the 92 subjects initially enrolled, four were not assessable for analysis: Two patients were later accepted to have LD, the data file of the one patient was not found during the final analysis, and one patient was ineligible due to diagnosed non-small-cell lung carcinoma on the histological review. The baseline patient and disease characteristics of these 88 eligible patients are listed in [Table - 1]. A median of six cycles (range, 1 to 6; 431 total cycles) of chemotherapy was administered. 58% (51/88) of the patients completed six courses. Course delay was observed in 11% of the total delivered cycles. Dose reductions took place in 3.2% of cycles as a result of hematological toxicities. 16 (18%) patients received second-line chemotherapy after relapse. The objective (complete plus partial) response rate was 69.4% [Table - 2]. As of September 2010, when the final analysis was conducted, the median OS was 9.0 months (95% CI, 8.09 - 9.90 months); 84 patients died. One patient lost to follow-up. Follow-up times were 79.7, 17.5, and 15.2 months in living patients. The 1-, 2-, and 3-year survival probability were 33.6, 5.3, and 1.3%, respectively [Figure - 1]. The median PFS in patients of 65 was 7.2 months (95% CI, 5.81 - 8.58 months), 12- and 18-month PFS rates were 10% and 1.5%, respectively [Figure - 1]. OS of the patient subgroups and toxic events are shown in [Table - 3] and [Table - 4], respectively. Grade 3/4 neutropenia was observed most frequently (57.9%). Febrile neutropenia was developed in 12 (13.7%) patients. There was no toxic death. Serum concentrations of lactate dehydrogenase (LDH) were found to be elevated in 58 (78%) of 74 patients. Serum levels of sodium were decreased in 11 (13%) of 82 patients. Serum levels of alkaline phosphatase were elevated in 43 (58%) of 74 patients. Discussion In our study, we evaluated the efficacy of carboplatin and etoposide in 88 patients with ED-SCLC. Overall median survival was 9.0 months. The overall rates of survival at 1 and 2 years were 33.5% and 5.0%, respectively [Figure - 1]. The median PFS was 7.2 months and 1-year PFS rate was 10%. The benefit of the PE regimen as first-line treatment is confirmed by two meta-analyses reporting a significant survival benefit of cisplatin-based chemotherapy compared with chemotherapy without cisplatin, contrary to the results of a third meta-analysis. Pujol et al.[4] evaluated 19 trials (4 054 evaluable patients) and reported that patients treated with a cisplatin-containing regimen had an increase in probability of being responders with an odds ratio (OR) of 1.35, 95% CI of 1.18 to 1.55, P < 10−5 , and benefited from a significant reduction of risk of death at 1 year with OR, 0.80; 95% CI, 0.69-0.93; P = 0.002 compared to the patients with chemotherapy involving other nonplatinum alkylating agents. In the systematic review of 7 173 patients from 36 trials, the authors of the ELCWP showed a survival benefit in favor of chemotherapy regimens, including etoposide alone or in combination with cisplatin. Nine trials (1 945 patients) compared a regimen including cisplatin and etoposide with a regimen without either drug. Hazard ratio with 95% CI was 0.57 (0.51-0.64, P < 0.001), in favor of the regimens containing both cisplatin and etoposide. [3] In conrast with these findings, the cochrane meta-analysis of 29 trials involving 5 530 patients showed no significant difference of platinum-based chemotherapy regimens in terms of survival at 6, 12, and 24 months or overall tumor response compared with non-platinum-based regimens. However, platinum-based chemotherapy regimens increased complete response rates at the cost of higher adverse events including nausea and vomiting, anemia, and thrombocytopenia toxicity. [17] There are some limitations in our study. The inclusion of patients with a PS of 3 is one of those. This made the target population heterogeneous. A further limitation of this study may be a long accrual period of nine-and-half years. We included the patients from a single unit in our hospital and consequently the accrual rate was slow. A possible bias in our study is not being able to determine the date of progression in patients of 23. However, OS cannot be compromised by that practice. In this study, tumor responses were evaluated according to WHO criteria instead of the Response Evaluation Criteria in Solid Tumors. This is due to start before 10 years of trial. The Hellenic Cooperative Oncology Group performed a randomized clinical trial comparing carboplatin (300 mg/m 2 on day 1) etoposide vs PE among 61 patients with ED-SCLC. [8] Response rates were similar with 50% responders (complete, 10%) for PE and 64% responders (complete, 16%) for carboplatin plus etoposide. Median survival rates in all study groups were 12.5 months for PE and 11.8 months for carboplatin plus etoposide. The patients who received carboplatin plus etoposide experienced significantly less toxicity, both nonhematologic and hematologic. WHO grade 3/4 leukopenia was seen in 37.5% /12.5% of the patients treated with PE in comparison with patients treated with carboplatin plus etoposide, who only experienced 10.3% /6.8% . Thrombocytopenia (WHO grade 4) occurred in only 6% of patients receiving PE and 4% of patients receiving carboplatin plus etoposide. Nausea and vomiting, nephrotoxicity, neurotoxicity, leukopenia, infection, mucositis, and allergic reactions were reported less frequently for patients in the carboplatin arm than for those in the cisplatin arm. Nausea and vomiting along with neurologic toxicities were significantly less in patients receiving carboplatin plus etoposide. WHO grade 2/3 nausea and vomiting occurred in 71% /4% of patients receiving etoposide and cisplatin, where nausea and vomiting only occurred in 25% /0% of patients receiving carboplatin plus etoposide (P = 0.0001). Neurologic toxicity (WHO grades 1/2) occurred in 41% /12% of patients receiving etoposide and cisplatin and only 18% /0% of patients receiving carboplatin plus etoposide, which was statistically significant (P0 = 0.0002). The other trial randomized 101 patients receiving their initial treatment for limited or extensive SCLC to either cisplatin or carboplatin in combination with etoposide. [11] There was no statistically significant difference in response rates (67.3% in the cisplatin group vs 57.2% in the carboplatin group). The median survival time in the cisplatin group was 12 months (95% CI, 10 - 17) vs 10 months (95% CI, 9-11) in the carboplatin group (P = 0.041). Grade 3 and 4 of hematological toxicities were more experienced in the carboplatin group (neutropenia grade 3, P < 0.05; thrombocytopenia grade 4, P < 0.01). Kunitoh study also included patients receiving initial treatment, but was restricted to 220 extensive disease SCLC patients who were elderly (age>/ = 70) or had "poor risk" characteristics. Both regimes were "well tolereted" with similar nause scores, but there was modestly more myelosupression with carboplatin (AUC, 5) than with cisplatin (25 mg/m 2 days 1, 2, and 3). Survival results were similar for both treatment arms in this study population. [12] Multiple retrospective studies have analyzed prognostic factors for SCLC. [18],[19],[20] A poor performance status and elevated LDH levels are consistently associated with poor survival. In our study population, multiple organ metastasis and elevated LDH levels were detected in patients of 36.4% and 78% (58/82), respectively. 17% of patients had poor performance status. Male gender and certain metastatic sites, such as liver, brain, and bone, as well as total number of metastatic sites involved were also found to be independent predictors of poor survival in the majority of studies. The prognostic significance of low serum sodium, elevated alkaline phosphatase, and older age is less clear. Liver metastases and multiple metastatic sites were identified as an adverse prognostic factor in our study group but not for brain metastases. Myelosupression, neutropenia in particular, was the most common toxic effect. Febrile neutropenia was developed in 12 (13.7%) patients. These patients were hospitalized and treated with antibiotic and G-CSF. Grade 1 to 2 anemia frequently occured. Significant trombocytopenia occured infrequently. Dose modifications as a result of hemotological toxicities were only performed in 3.2% of cycles. Nonhematological toxicities were mild in all patients. Grade 3/4 nonhematological toxicities were not observed except alopecia. Although we were unable to retrieve information on patient quality-of-life in this study, most toxicities were tolerable and the treatment compliance was also favorable. Approximately two-thirds of the patients received all six cycles of treatment. Overall median survival is 9.0 months in our patient group. This survival time seems dismal; however, What is the situation in other carboplatin plus etoposide trials? Socinski et al. designed the trial to detect noninferority of pemetrexed (Pem; 500 mg/m 2 ) plus carboplatin (AUC 5) as compared with etoposide (100 mg/m 2 on days 1 through 3) and carboplatin (AUC 5). In the final analysis, PemC was inferior to carboplatin plus etoposide for OS (median, 8.1 vs 10.6 months; P < 0.01) and PFS (median, 3.8 vs 5.4 months; P < 0.01). [21] Nearly similar outcomes were observed in current trial compared with etoposide-carboplatin arm of Socinski et al. Objective response rate were moderately higher for our patients than for those on carboplatin plus etoposide arm of Socinski trial (52% vs 69.4%). Complete response rate was also higher for our patients (23.9% vs 0.3%). But, higher response rates have failed to improve survival. Febrile neutropenia also occured more often in the AUC 6 dose of carboplatin in present trial (13.7% vs 4.5%). Heigener et al. compared dose-intensified CE with the supplementation of G-CSF and conventional CE (carboplatin AUC 5 on day 1 IV and etoposide 140 mg/m 2 IV on days 1-3, q28 days). Median survival in the conventional group and the dose-intensified group were 11.2 months and 11.7 months, respectively. [22] PFS was 6.7 months and 7.4 months, respectively. There was no statistically significant difference between these groups. The favorable OS rate in this trial by Heigener et al. may be attributable to patient selection. Although the proportion of the poor prognosis factor of the patients was not specified, nearly all of the patients had a good PS in contrast to our trial. Some 3-drug combinations showed promising results with dose intensifications. In a trial by Buchholz et al., 83 patients were randomized to receive ifosfamide, carboplatin, and etoposide in a 4-week (Standard chemotherapy, SCT) vs 2-week schedule (Intensified chemotherapy, ICT) with filgrastim-supported sequential reinfusion of peripheral blood progenitor cells every 14 days. [23] Median survival was significantly improved with ICT (30.3 months) vs SCT (18.5 months); 2-year survival was 55% for ICT and 39% for SCT. Time to progression was significantly improved, with 15 months for ICT vs 11.1 months for SCT. In a trial by EORTC, 224 patients were randomized to receive cyclophosphamide, doxorubucine, and etoposide (CDE) every 3 weeks or every 2 weeks with G-CSF support. [24] A 70% increase CDE actual dose intensity does not translate into an improved outcome in SCLC patients. The optimal drug doses remain unclear with several studies suggesting a possible benefit. The dose of carboplatin of AUC 6 (day 1) and etoposide of 100 mg/m 2 (days 1, 2, and 3) is an active and tolerable regimen in patients with ED-SCLC. The obtained survival results in our study are comparable with historical results of the cisplatin in combination with etoposide in previously untreated patients with ED-SCLC. Prospective randomized studies of carboplatin plus etoposide are warranted. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11125f1.jpg] [cn11125t2.jpg] [cn11125t1.jpg] [cn11125t3.jpg] [cn11125t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}