 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
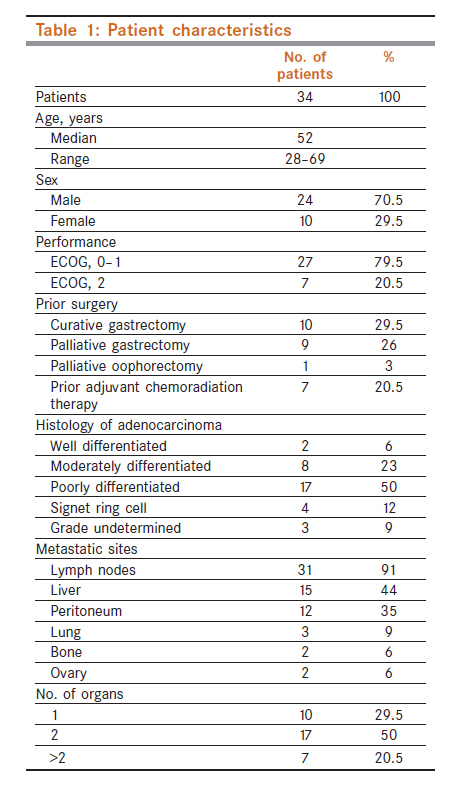
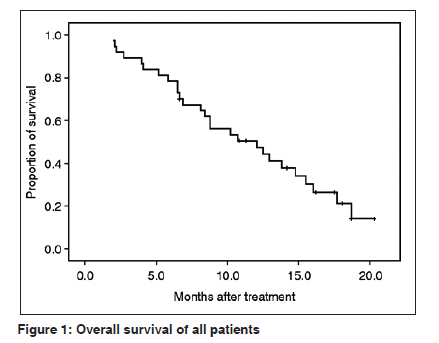
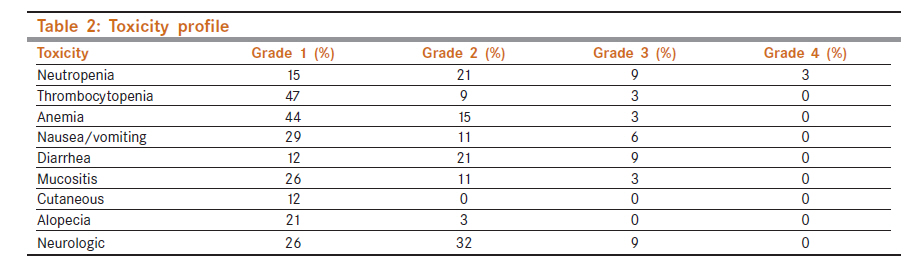
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 460-465 Gastrointestinal - Original Article FOLFOX (oxaliplatin and 5fluorouracil/leucovorin) in patients with untreated metastatic gastric adenocarcinoma Phase II study HA Mohammad, FM Magdy, OM Mahmoud Department of Surgery, Erfan Hospital, Shahid Bakhshayesh St., Western-Sarv St., Saadat Abad, Tehran, Iran Code Number: cn11126 PMID: 22293261 Abstract Background: Oxaliplatin has shown promising activity in metastatic gastric cancer (MGC) and has synergism with 5 fluorouracil. This phase II study was performed to evaluate the efficacy and safety of FOLFOX4 regimen in MGC. Keywords: Chemotherapy, gastric, oxaliplatin Introduction Gastric cancer is the most frequent cancer-related cause of death after lung cancer. [1] Metastatic gastric cancer (MGC) remains a therapeutic challenge for medical oncologists due to poor prognosis. Several randomized phase III trials comparing combination chemotherapy such as 5fluorouracil (5FU), doxorubicin, and mitomycin or 5FU, doxorubicin and highdose methotrexate with best supportive care have demonstrated significantly prolonged overall survival (OS) (8-10 months) for chemotherapy group as compared to best supportive care alone (3-5 months). [2],[3] Since then, various combination chemotherapy regimens were tested in phase II or phase III trials in MGC. A phase III trial comparing docetaxel,cisplatinand5FU (DCF) to the reference arm of cisplatinand5FU (CF) showed a significant superiority of DCF in terms of survival (9.2 versus 8.6 months), time to progression (TTP) (5.6 versus 3.7 months), and response rate (RR) (37% versus 25%) than CF arm. [4] However, because DCF regimen was associated with high incidence of grade 3 and 4 toxic effects, the regimen has not yet been widely accepted as the standard first line chemotherapy for gastric cancer patients. Thus, the optimum front line chemotherapy regimen should be extensively investigated in these patients to improve survival. Oxaliplatin has shown a notable activity against colorectal cancer in combination with 5FU and leucovorin which led to several phase II trials in gastric cancer. The oxaliplatin/5FU/leucovorin regimen in different schedules yielded RRs in the range of 38-52% with median survival time from 8 to 11 months with tolerable toxicity. [5],[6],[7],[8] On the basis of these encouraging results we conducted a phase II study in order to assess the efficacy and safety of the FOLFOX4 as a front line chemotherapy in patients with MGC. Materials and Methods Eligible patients were required to have histologically confirmed metastatic adenocarcinoma of the stomach, at least one bi-dimensionally measurable lesion according to Response Evaluation Criteria in Solid Tumors (RECIST) criteria. [9] No previous chemotherapy or radiotherapy, age between 18 and 70 years, an Eastern Cooperative Oncology Group performance status of two or less, adequate hematological parameters [hemoglobin ≥9.0 g/dl, absolute neutrophil count (ANC) ≥ 1500 per μl, platelet count ≥100 000 per μl, renal function (creatinine clearance by Cockroft formula ≥50 ml/min or creatinine ≤1.5 mg/dl), and liver parameters [aspartate aminotransferase, alanine aminotransferase ≤3× the upper limits of normal (ULN), total bilirubin <2× ULN]. Patients who received adjuvant chemotherapy >6 months from the date of study entry and not include oxaliplatin were eligible for the study. Patients with metastasis to the central nervous system were excluded. All participants provided written informed consent before they entered the study. Treatment FOLFOX4 was administered every 2 weeks as oxaliplatin 85 mg/m 2 IV infusion on day 1 and leucovorin 200 mg/m 2 IV infusion followed by fluorouracil 400 mg/m 2 IV bolus and 600 mg/m 2 22hour continuous infusion on days 1 and 2. Treatment was administered until progression or unacceptable toxicity, patient′s refusal or for a maximum of 12 cycles. Antiemetic prophylaxis was given according to the local protocols including 5HT3 antagonists and dexamethasone were given before chemotherapy. Both drugs was delayed as long as there was diarrhea or mucositis of Common Toxicity Criteria (CTC) grade 1 or greater, neutropenia <1500 per μl or thrombocytopenia <100, 000 per μl. Also both drugs were reduced by 25% of the previous dose in case of grade 3/4 toxicities. Efficacy assessment The primary objective of the study was RR and secondary objectives were toxicity, OS and TTP. Pretreatment evaluation included history and physical examination, complete blood cell count with differentials, chemistry,, computed tomography (CT) scan of abdomen and pelvis, chest Xray or CT and any other diagnostic procedures as clinically indicated. During treatment, a history taking, physical examination including toxicity assessment, complete blood cell count and chemistry were carried out every 2 weeks before each cycle. Appropriate imaging studies including abdominal and pelvis CT scan were carried out every 4 cycles (8 weeks) to evaluate treatment response, or sooner if needed for documentation of disease progression. Responses were to be confirmed by subsequent CT scans 4-6 weeks after the initial response documentation. Patients were assessed every 3 months for disease progression following the completion of the chemotherapy. Responses were classified according to RECIST criteria. [9] Considered assessable for response if early disease progression occurred or if they had received at least two cycles of treatment, with at least one follow up tumor assessment. TTP was calculated from the first day of treatment to the date on which disease progression was first documented or of the last follow up. OS was calculated from the first day of treatment to the date of death or last follow up. Toxicity was monitored according to the National Cancer Institute (NCI) CTC scale version 3.0. Statistical considerations The expected number of patients for this study was calculated according to a Simon optimal two stage design. An interim analysis was carried out if over three patients among the first 17 patients have objective response; this study is regarded to be adequate to proceed further and to enroll more 17 patients assuming P 0 of 15%, P 1 of 35%, α-error of 0.05 and B-error of 0.20. Thirty four eligible patients were required to evaluate the activity of this combination. Descriptive statistics was reported as proportions and medians. Kaplan-Meier estimates were used in the analysis of time to event variable and the 95% confidence interval (CI) for the median time to event was computed. The dose intensity (DI) was calculated as the ratio of the total dose in milligrams per square meter of the patient divided by the total treatment duration expressed in days. The relative DI was calculated as the ratio of the DI actually delivered to the DI planned by the protocol. Results From August 2007 to June 2010, 34 patients were enrolled. The baseline characteristics are listed in [Table - 1]. The median age was 52 years (range 28-69 years). All patients had a histologically proven adenocarcinoma of the stomach two of them had primary tumors at the gastroesophageal junction. Thirty one (91%) had distant lymph node metastases, 15 (44%) liver metastases and 24 (70.5%) had two or more sites of metastases. Of the 10 patients with single organ involvement, 7 patients had metastasis limited to lymph nodes however the nodal involvements occurred in left para-aortic, aortocaval, retrocaval, retropancreatic and supraclavicular lymph nodes. Two patients had metastatic tumors to the ovaries. All patients had metastatic disease at the time of study entry. In total, 293 cycles were administered with a median of 8 cycles per patient (range 1-12 cycles). The delivered relative dose intensities (DIs) were 82% for oxaliplatin and 83% for 5-FU. Response Thitty three (97%) of 34 patients were assessable for response. One patient was not assessable but was included in the intent to treat analysis. This patient stopped chemotherapy after one cycle because of patients′ refusals. The overall response rate (ORR) was 53% (95% CI 4270%). One patient (3%) had complete response (CR) and 17 patients (50%) had partial response (PR) and 6 patients (18%) had stable disease. All CRs and PRs were confirmed at least 4 weeks later. The extent of disease (patients with one organ, two organs or more than two organs involvement) did not influence RRs. Upon disease progression 17 patients (50%) received a second line treatment including docetaxel/cisplatin (n=10) and irinotecan, 5FU, leucovorin chemotherapy (n=7). Survival All patients were included in the survival analysis.The median follow-up duration was 12.8 months (range 6.7-18.7 months). The median OS was 12.1 months (95% CI = 7.0-17.1 months) [Figure - 1] and the median TTP was 9.4 month. All patients were assessable for safety. Toxic effects observed during the study are listed in [Table - 2]. The most common toxic effects were neutropenia,neurotoxcities . Most patients experienced neutropenia during their course of therapy with 12% of patients (n=4) for grade 3/4. However there were only one episodes of grade 3 neutropenic fever of all cycles in one patient. There was no treatment-related death or life-threatening neutropenic fever. Nonhematological toxic effects of grade 3/4 occurred in <10% of cycles. Grade 3 nausea and vomiting occurred in 6% of patients. Although peripheral neuropathy was commonly observed, most patients had mild (grade 1 in 26%, grade 2 in 32% of patients) and three patients (9%) had severe peripheral neuropathy requiring treatment interruptions.Grade 3 diarrhea occurred in three (9%) patients. Of the 34 patients who received more than one cycle, 14 (41%) had at least one dose reduction in a total of 24 cycles (8%). Seven patients (20.5 %) had a dose reduction in both oxaliplatin and 5-FU. Four (12%) patients were delayed >1 week because of nonhematological toxic effects. Three patients were discontinued from the study due to grade 3 neurotoxicities after 11 cycles in one patient and 10 cycles in the other two patients effects (cumulative oxaliplatin dose of ≥ 850 mg/m 2 ). Also treatment was discontinued in nine patients due to progression of the disease. Discussion MGC remains an incurable disease with poor prognosis although randomized trials had demonstrated that chemotherapy provides survival and symptomatic benefits in patients with advanced gastric cancer over supportive care alone, [2],[3] these benefits were fairly modest. In the largest phase III trial (V-325) compared DCF with the reference regimen of CF demonstrated significant superiority of DCF in terms of survival (9.2 versus 8.6 months), TTP (5.6 versus 3.7 months) and RR (37% versus 25%) than CF arm. [4] Because DCF is an intensive combination with the incidence of grade 3/4 neutropenia of 82%, the benefit to risk ratio should be cautiously determined in incorporating the regimen in practice especially in an elderly population.Oxaliplatin in various combinations with 5-FU and leucovorin were tried as first line treatments for advanced gastric cancer, and the reported RRs were 38-52%. [5],[6],[7],[8] On the contrary to colorectal cancer, in vitro antitumor activity is reported to have a strict sequence dependency of oxaliplatin followed by 5FU in gastric cancer which was the basis of this protocol development. [10] Therefore, we studied the combination of 5-FU with oxaliplatin (FOLFOX4) that could be administered more easily in clinical practies for colorectal cancer patients [11] in order to develop a potentially more efficacious front-line chemotherapy of with acceptable toxicity. In this study FOLFOX4 achieved an ORR of 53% with 3% had CR and median OS of 12.1 months in patients with MGC and thus it compared favorably with the reported efficacy of common two- or three-drug combinations including FAMTX. [4] ELF. [12],[13] FAP (5-FU, doxorubicin and cisplatin) [14] and FP. [15] Also, the outcome of the present study seems to be favorably to the results of other previous studies using oxaliplatin, leucovorin and 5FU in different schedules-containing regimens for advanced gastric cancer. Westren studies with this combination have used a higher or lower dose of each drug to study the efficacy and toxic effects. Lauvet et al[5] evaluated the efficacy and tolerance of FOLFOX6 combination with higher dose (oxaliplatin 100 mg/m 2 with 5-FU 400 mg/m 2 bolus followed by 600 mg/m 2 22h infusion for 2 days) in 54 MGC patients and demonstrated a RR of 44.9%, TTP was 6.2 months and OS was 8.6 months with high toxicity profile (Grade 3/4 neutropenia, leukopenia, thrombocytopenia and anemia occurred in 38%, 19%, 4% and 11% of patients, respectively, and febrile neutropenia occurred in six patients (one episode each). Grade 3 peripheral neuropathy occurred in 21% of patients. Seven patients withdrew because of treatment-related toxicity), although there is little evidence that a higher oxaliplatin dose guarantees higher. RR Jeong et al[16] assessed the feasibility of FLOX combination regimen with reduced dose (oxaliplatin 75 mg/m 2 on day 1, 5-FU 1000 mg/m 2 on days 1-3 and leucovorin 20 mg/m 2 on days 1-3 every 3 weeks). In 52 patients with MGC, the median OS was 6.6 months (95% CI 4.5-8.8) and the median progression-free survival was 2.5 months (95% CI 1.9-3.0). The RR was 4% (95% CI 0-9%), and the disease control rate was 48% (95% CI 34-62%). The most common toxic effects of grade 3/4 were neutropenia (16%) and vomiting (6%).in other study by Al-Batran et al : [8] Forty-one previously untreated patients withMGC received modified dose of 5 FU (without IV bolus) 2.6 g/m 2 (24-hour continuous infusion), FA 500 mg/m 2 (2 hour intravenous infusion) and oxaliplatin 85 mg/m 2 (2-hour intravenous infusion) every 2 weeks for 6 weeks. The ORR was 43%, Stable disease was observed in 12 patients (32%) and progressive disease in nine patients (24%). The median OS was 9.6 months and the median TTP was 5.6 months (range 1.3-22.3 months). In this study, the ORR was 53% by intent to treat analysis with one CR and 17 PR. All responses were confirmed by a second assessment at least 4 weeks later. Although seven patients had metastases confined to lymph nodes only, these lymph nodes were all located in distant sites. Hence, the observed RR of 53% is among the highest RRs reported for gastric cancer using this combination. Accordingly, the median survival time (12.1 months) was longer compared with other phase II using this combination (range 6.6-8.6 months). [15],[16] Although the median follow-up time is 12.8 months at the time of the analysis. The results reported here was improved by the addition of a third active drug like irinotecan 150 mg/m 2 to this protocol as in the study of JLee et al: [17] Resulted in ORRof 66.7% in 48 patients with untreated MGC, the median OS of 14.8 months and the median TTP was 9.6 months. Most common grade 3/4 toxic effects were neutropenia (12% of all cycles) and emesis (8% of all cycles). Grade 2 peripheral neuropathy occurred in five patients. One (2%) patient had severe tumor bleeding and five (10%) patients experienced grade 3 diarrhea. Also the results may be improved by the addition of targeted therapy like Trastuzmab in over expressed HER 2 gastric cancer. Understanding the biology of gastric cancer may result in better targets or cellular pathways that can be modified or blocked by therapeutic intervention. Improvements in clinical trial design and the introduction of molecular surrogates to clinical research will also lead to the development of better treatments. Both clinical and biological research will become more important. The FOLFOX4 regimen in this study demonstrated tolerable toxicity profile. The incidence of grade 3/4 neutropenia reported was 12% of patients, neutropenia was usually short lasting and only one patient has one episode of neutropenic fever. The regimen, however, showed 9% of grade 3 neuropathy which led to discontinuations of the drug in three (9%) patients and this toxicities′ profile seemed to be favorable to the other studies using this combination as mentioned above. [15],[16] So this disparity of the results of our study which appears favorable to the results of western studies may be related to biological behaviors of our patients in Saudi Arabia (Asian country), this disparity in the results was reported in most of the studies of the west and east countries, this a question is needed to be answer in large randomized studies. [18] In total, 293 cycles were administered with a median of 8 cycles per patient (range 1-12 cycles). The delivered relative DIs were 82% for oxaliplatin and 83% for 5FU which were comparable to phase II study of similar regimen in colon cancer patients. [11] In conclusion, FOLFOX4 combination is a well tolerated treatment modality with very promising activity in untreated MGC patients. Further randomized phase II or III clinical trials are necessary for determining the optimal dose and schedule of a combination of oxaliplatin, leucovorin and 5FU in gastric cancer. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11126t2.jpg] [cn11126t1.jpg] [cn11126f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}