 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 466-470 Gastrointestinal - Original Article Clinicopathologic spectrum of gastro intestinal stromal tumours - Experience at a tertiary care center G Ravikumar, IY Kalegowda, A Ananthamurthy Department of Pathology, St.John's Medical College and Hospital, Bangalore, India Code Number: cn11127 PMID: 22293262 Abstract Context: Accurate diagnosis of Gastrointestinal stromal tumors (GISTs) and categorization of risk groups is crucial in the wake of targeted drug therapy. Keywords: c-KIT, CD117, gastrointestinal stromal tumor, immunohistochemistry, pathology Introduction Gastrointestinal stromal tumors (GISTs) are the most frequent mesenchymal tumors of the gastrointestinal tract. [1] These are Kit / PDGFRA mutation -driven mesenchymal tumours that can occur anywhere in the gastrointestinal tract, most commonly in the stomach and small intestine. The availability of Kit/ PDGFRA tyrosine kinase inhibitor Imatinib mesylate and other newer drugs for metastatic and unresectable GISTs has remarkably improved the prognosis and survival rates for patients with these tumours. [2],[3] GISTs are diagnosed by virtue of characteristic histologic features in conjunction with immunohistochemistry, complemented with gene mutation analysis. Approximately 80−85% of GISTs harbor activating mutations of Kit tyrosine kinase (CD117). [4] An insight into the clinicopathologic features and accurate risk categorization is important in this era of targeted drug therapy. Although there has been a virtual explosion of data regarding GISTs in the last decade, there is limited published information in the South Asian region, which prompted us to undertake this study. Aims and Objectives To describe the demographic characteristics, frequency of risk categories, histopathology, and immunoprofile of cases of GISTs that were encountered in a tertiary care center. Materials and Methods Twenty cases of CD117-positive GISTs diagnosed between January 2006 and March 2009 who underwent complete surgical resection were included in this retrospective study. The case files and slides were retrieved and reviewed, and follow-up information was obtained wherever available. The demographic details, organ distribution, gross morphology, histology, and immunohistochemical profiles were studied. Each case was examined for the following histologic features:
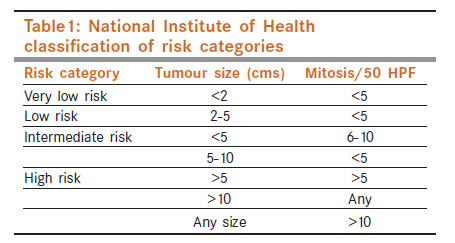
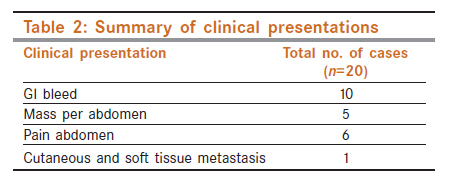
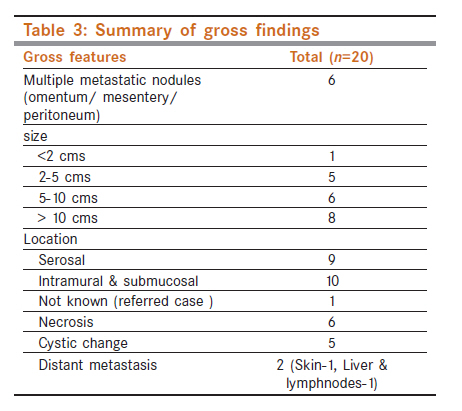
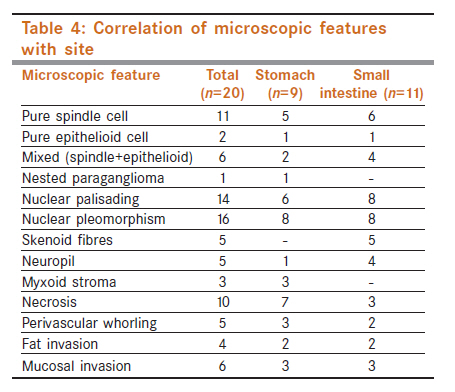
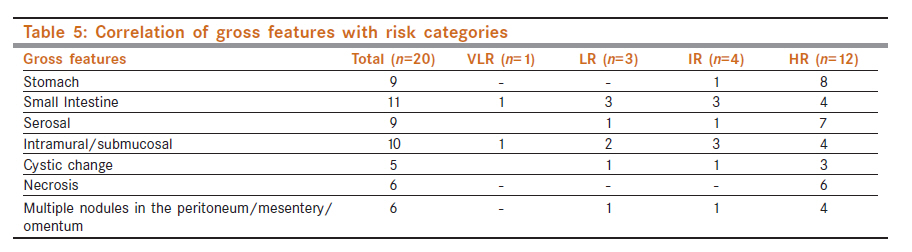
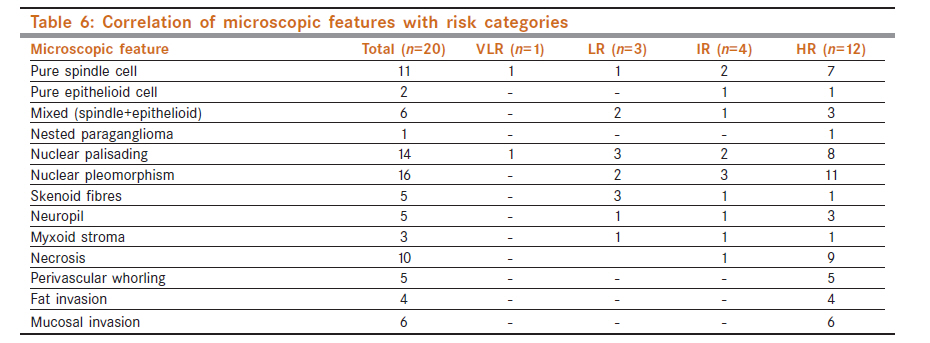
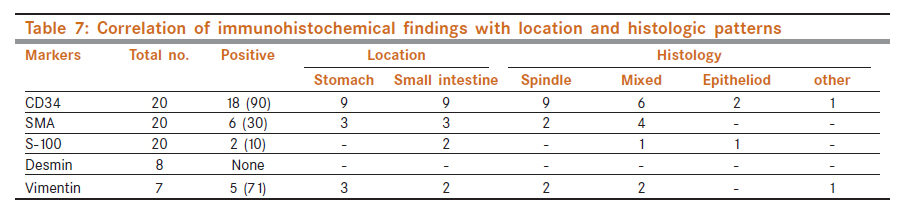
Cases were assigned into very low, low, intermediate, and high-risk groups based on the National Institute of Health (NIH), consensus classification [Table - 1]. [1] A panel of immunologic markers in addition to CD-117 such as CD-34, smooth muscle actin (SMA), and S-100 were done on all the cases and the staining was analyzed with regard to location, intensity, and percentage of tumor cells, which stained positive. In addition, Desmin and vimentin were done in some of the cases. Results Out of the 20 cases, there were 15 males (75%) and 5 females (25%). The mean age of presentation was 53.6 years in males and 47.6 years in females. The most common presenting symptom was gastrointestinal bleeding which was seen in 10 cases, 8 of whom typically described black colored stools. The other modes of clinical presentations are summarized in [Table - 2]. Interestingly, one case, which presented with multiple cutaneous nodules on retrospective analysis, turned out to be metastasis from a gastric GIST. Another case presented as distant metastasis to the liver and lymph nodes. Data on follow-up was available for 56% of the cases with the follow up period ranging from 2 to 18 months (median follow-up = 10 months). Four patients were started on Imatinib mesylate during this period. Although one of the cases who presented to us was a recurrent GIST, none of the other cases had recurrences during our follow-up period. The most common site of occurrence was the small intestine (11 cases), followed by stomach (9 cases). All were complete resection specimens and the tumor size ranged from 0.5-30cms (mean: 10.6 cm). In 8 cases (40%), the tumors were >10 cms in greatest dimension. Six cases (33%) had multiple metastatic nodules in the peritoneum, mesentery, or omentum. The cut surface of all the tumors were grey white and solid [Figure - 1], and in six cases (all of which were high-risk category) frank necrosis was discernible. Distant metastasis was seen in two cases. The details of the gross findings are summarized in [Table - 3]. On microscopy, the spindle cell pattern [Figure - 2]a was the most common histological pattern observed in eleven cases (55%), followed by a mixed spindle and epithelioid cell morphology in seven cases (35%). There were two cases displaying pure epithelioid cell morphology [Figure - 2]b and a nested paraganglioma-like pattern was observed in a single case [Figure - 2]c. Necrosis was seen in 10 cases of which 90% belonged to the high-risk category. Mild to moderate nuclear pleomorphism, and nuclear palisading [Figure - 2]d were other features frequently noticed (16 and 14 cases, respectively). Stromal skenoid fibers [Figure - 2]e were seen in five cases, all of which were small intestinal GISTs. Juxtanuclear cytoplasmic vacuoles and myxoid stromal change were rarely observed (two and three cases, respectively). [Table - 4] summarizes the microscopic features with regard to site. Risk categorization based on the size of the tumor and mitosis revealed that most of the tumors belonged to the high risk (60%) or the intermediate risk (20%) category, while a few fell into the low risk (15%) and very low risk category (5%). There was no significant difference in the mean age of presentation in the various risk categories. Also there was no significant difference in the occurrence of high risk cases in men and women. Gastric GISTs, location in the serosa, and presence of metastatic nodules in the peritoneum/ mesentery/ omentum were more commonly encountered in the high-risk group. The microscopic features observed exclusively in high-risk categories were nuclear pleomorphism, perivascular whorling [Figure - 2]f, mucosal invasion, and fat invasion. Spindle cell pattern, nuclear palisading, pleomorphism, and necrosis were also more common in the high-risk groups. The correlation of gross and microscopic findings with risk categories are summarized in [Table - 5] and [Table - 6], respectively. CD117 positivity was one of the inclusion criteria in this study. CD 34, SMA and S-100 were done in all cases and were positive in 18 (90%), 6 (30%), and 2(10%) cases, respectively. In addition, Desmin and vimentin were done in eight and seven cases, respectively. Desmin was consistently negative in all the cases and vimentin was positive in five of the seven cases. [Table - 7] portrays the immunoprofile of all the cases. Discussion GISTs, which at one time was a poorly defined entity has now evolved into a distinct group of mesenchymal tumors. With the advent of kinase-targeted therapies, which have proved to be promising, it is crucial for the pathologist to diagnose and accurately categorize the risk group for the optimum management of these cases. In the present study, there was a marked male predominance comparable to other South Asian studies, [5],[6] although Western literature claims an equal sex predilection. [2],[4],[7] The mean age of presentation was 52 years, which was about a decade earlier than that reported in the western population. [2],[4],[6] Another study from southern India also reports an earlier mean age of presentation (48.2 yrs) similar to our study.- [8] Gastrointestinal bleeding, probably due to surface ulceration, was the most common clinical presentation. Other GIST cohort studies have reported abdominal pain, abdominal mass, early satiety, bloating, and fatigue related to anemia as presenting symptoms. [2],[5],[6] Small intestine and stomach were the two sites commonly involved by the tumor with an almost equal incidence in both. In contrast, other studies have reported a slightly higher incidence of gastric GISTs. Also, most of our gastric GISTs (89%) belonged to the high-risk group unlike other western studies. [1] The location of GISTs within the bowel wall may be serosal, intramural or sub mucosal with a solid, grey- white cut surface. The presence of gross necrosis is usually associated with high-risk groups as seen in our cases. About 20−25% of gastric GISTs and 40−50% of small intestinal GISTs are clinically malignant. The common sites of metastasis are the abdominal cavity and liver. Rarely bones, soft tissue and skin may be involved. [9],[10] We had two cases with distant metastasis of which one was an extremely rare case presenting as a cutaneous nodule with an epithelioid cell morphology and exhibiting CD117 positivity. On retrospective analysis, it was found to be a metastasis from a gastric GIST. The other case showed metastasis to the liver and lymph nodes. In addition, six cases showed multiple peritoneal and omental metastases, four of these belonged to the high-risk category. Most of our cases were in the high-risk category, which is similar to the study by Rauf et al. [5] Other studies report a lesser incidence of high-risk cases. This finding may be attributed to referral bias, since our institute is a tertiary care center. Various histologic patterns have been described in GISTs; the commonest being the spindle cell pattern, followed by epithelioid pattern and mixed pattern.- [3] Our study showed mixed pattern to be the second most common pattern. Rarely one may encounter a nested paraganglioma like/ carcinoid like pattern. Tumor histology has been correlated with outcomes in a few GIST cohorts. [7],[11] Although it is said that pure epithelioid pattern and mixed patterns are more common in the stomach with a poorer prognosis, we could not substantiate these findings as the number of cases in our study were too small with inadequate follow-up. Nuclear palisading was a common feature in our series. Skenoid fibres and neuropil was predominantly observed in small intestinal GISTs as seen in other studies. [2],[3] A prominent myxoid stroma may be seen in some cases. We observed that perivascular whorling of cells was a feature seen exclusively in high risk categories. This association has not been described previously. The other common features associated with high-risk behavior were necrosis, nuclear pleomorphism, mucosal invasion, and fat invasion which have been described as factors associated with poor outcome. According to literature, 80−85% of GISTs are CD117 positive, 60-70% are positive for CD34, 30-40% for SMA, 5% for S-100, and 1-2 % for Desmin . [ 2],[3],[4] In our study, as per the inclusion criteria all the cases were CD117 positive. The percentage of cases positive for CD34 and S-100 was much higher (90% and 10% respectively). Most cases of CD34 positive GISTs had spindle cell morphology and did not show any site predilection . Consistent Desmin negativity and low S-100 positivity was concurrent with other studies. Conclusions The present study exhaustively elucidates the various gross, histologic, and immunohistochemical features in association with the various risk groups along with demographic details of GISTs in a series of twenty patients in our clinical set-up. In our practice, GISTs occur a decade earlier than in the western population, mostly in males and mostly belong to the high-risk group. Most GISTs located in the stomach belong to the high-risk group. Although GIT symptoms such as bleeding is a common clinical presentation, rarely one may encounter unusual presentations (such as cutaneous nodules) due to metastases. Presence of metastatic nodules in the peritoneum and omentum is also a common feature in GISTs. Spindle cell morphology is common, although other patterns such as epithelioid and paraganglioma like features may be admixed. Positive CD34 staining is a useful adjunct in the diagnosis of GIST and does not show any site predilection. SMA and S-100 may be positive sometimes. Desmin is usually negative. Gross necrosis, presence of multiple metastatic nodules in the mesentery/ omentum/ peritoneum, nuclear pleomorphism, perivascular whorling, mucosal, and fat invasion are commonly observed in the high-risk group and probably portrays a bad prognosis. As this study involved a small cohort, further larger studies with adequate follow-up are warranted to validate these parameters as independent prognostic factors. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11127t3.jpg] [cn11127f2.jpg] [cn11127t6.jpg] [cn11127f1.jpg] [cn11127t7.jpg] [cn11127t4.jpg] [cn11127t1.jpg] [cn11127t5.jpg] [cn11127t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}