 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
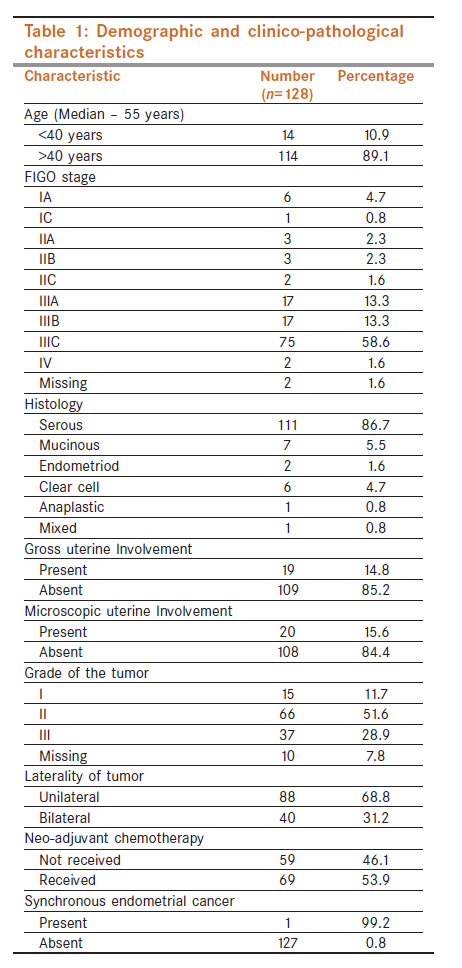
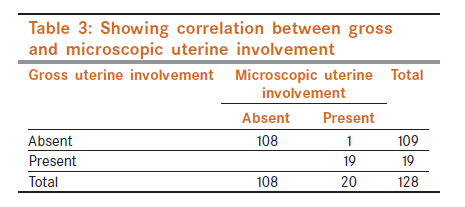
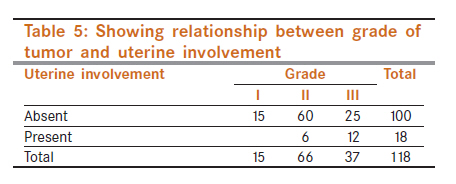
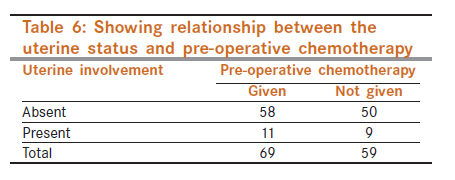
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 471-476 Gynaecological - Original Article Is hysterectomy needed in ovarian cancer? K Chitrathara1, ZA Sheikh1, DK Vijaykumar1, S Kuriakose2, R Anupama2, M Nandeesh1 1 Department of Surgical Oncology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India Code Number: cn11128 PMID: 22293263 Abstract Context: Hysterectomy is an integral part of ovarian cancer surgery. The authors have evaluated the uterine involvement in ovarian cancer in this study. Keywords: Conservative surgery, epithelial ovarian cancer, ovarian cancer Introduction Ovarian cancer is the third leading cancer among women in India, trailing behind cervix and breast cancer. [1] It carries worst prognosis amongst all the gynecological malignancies. Most patients present with advanced disease, which is managed by surgery integrated with platinum-based chemotherapy. [2] Traditional surgical management involves a hysterectomy with bilateral salpingo-oophorectomy, infracolic omentectomy, excision of metastatic peritoneal deposits (which may entail excision of underlying viscus) ± para-aortic lymph node sampling (wherever appropriate). [3] Surgical management aims solely on attaining an optimal cytoreduction. [3] A conservative fertility preserving surgical approach has been proven to be oncologically safe and effective in certain patient groups, viz., those with early (stage IA/B) low-grade tumors and germ cell and borderline tumors. [4] The basic aim of surgery is to remove the primary tumor and gross metastatic deposits. The benefit of removing uterus, when it is free of disease is questionable, since its preservation does not affect survival as has been proven by utilizing conservative approaches in the above-mentioned situations. This study was undertaken to evaluate the pathological involvement of uterus in epithelial ovarian cancer (EOC) with an aim to question the need for routine hysterectomy in ovarian cancer surgery. The aim of this study was to evaluate the pathological involvement of the uterus in ovarian cancer. The key question asked was whether uterus is involved in ovarian cancer and if yes, then how frequently and further can we predict the microscopic involvement of uterus from gross examination. Henceforth in this article, the term "uterine involvement" means both gross and microscopic involvement. Materials and Methods A retrospective chart review of the data of all the patients treated in a dedicated gynecologic oncology unit at cancer institute of Amrita Institute of Medical Sciences at Kochi in Kerala was done. All patients diagnosed to have EOC and operated from 2004 January to 2008 June were analyzed. The data regarding the clinical, demographic, operative, and pathological findings was retrieved from the electronic medical records (EMRs) stored in the institutional server. Only those patients who had undergone hysterectomy as part of their cytoreductive/staging surgery were included in the study. Patients with germ cell or borderline histology and those with previous history of hysterectomy were excluded. The data thus collected was tabulated and analyzed in the statistical software SPSS 11. Chi-square test was used to check for significance. Results From January 2004 to June 2008, 210 patients of carcinoma ovary were operated in our institute. Out of these, 128 patients were eligible for our study. The various demographic and clinico-pathological characteristics of these patients are tabulated in [Table - 1]. Most of the patients were above 40 years of age, with only 14 patients (10.9%) being younger than 40 years. The median age of presentation was 55 years (range 20-75 years). Majority of the patients presented at an advanced stage, with 88% (n=126) being FIGO III or above at diagnosis. Serous histology was the predominant tumor type (86.7%), followed by mucinous (5.5%) and clear cell (4.7%), with endometriod, anaplastic and mixed histologies contributing a few numbers. Gross uterine involvement was reported only in 19 (14.8%) patients. Microscopic uterine disease was seen in all patients who had gross involvement of the uterus and in one patient who had grossly free uterus. Most of the patients had either intermediate (n=66) or high-grade (n=37) tumors. In 10 patients the grade of the tumor was not reported. Almost equal number of patients underwent surgery either upfront (46.1%) or after receiving neo-adjuvant chemotherapy (NACT) (53.9%). Incidental synchronous endometrial cancer was noted only in one patient (poorly differentiated adenocarcinoma in an endometrial polyp, with moderately different serous papillary tumor in ovary). On analyzing the pattern of uterine involvement (n=20), it was noted that six patients had only serosal involvement and 13 (10%) patients had involvement of myometrium and none of these had endometrial involvement, whereas one patient who had no gross uterine disease had an endometrial polyp with serous papillary deposits on surface on microscopy. All the patients with myometrial involvement had it due to local infiltration from outside; so the total number of patients with serosal involvement was 19 (15%). The correlation between microscopic uterine involvement and stage [Table - 2], gross uterine involvement [Table - 3], histology [Table - 4], grade of tumor [Table - 5], and pre-operative chemotherapy [Table - 6] was analyzed by Chi-square test. Grade of the tumor and gross uterine involvement were the only factors that showed statistically significant correlation with the microscopic uterine involvement (P=0.001 and 0.03, respectively). Of the 15 patients with Grade I tumors none had uterine involvement whereas 6 out of 66 patients with Grade II tumors (9.1%) and 12 out of 37 patients with Grade III tumors (32.4%) had uterine involvement. This shows a significant predilection for high-grade tumors to affect the uterus. Involvement of the uterus was found to be independent of the stage of disease (P=0.5), the histopathological type of tumor (P=0.27) and preoperative chemotherapy (P=0.34). Discussion Carcinoma ovary is the 9th most common cancer and ranks 5th in cancer-related deaths in USA. [5] In India ovarian cancer contributes a significant cancer burden and is the third leading cancer in women. [1] Most patients have advanced disease at presentation, which is managed by surgery combined with platinum-based chemotherapy. Past decade has seen significant advances in chemotherapy, which has resulted in improved survival and more effective treatment of relapsed disease. The standard surgical approach involves a vertical midline incision, which provides adequate exposure of the upper abdomen and pelvis. A total abdominal hysterectomy and bilateral salpingo-oophorectomy, along with careful examination of all peritoneal surfaces, omentectomy, biopsy of para-aortic lymph nodes when appropriate, random biopsies of clinically uninvolved areas and peritoneal washings are part of the surgical protocol. Biopsy of the para-aortic nodes is especially important in patients with early disease, since such patients may turn out to have more advanced disease. [6] In advanced disease, cytoreduction is the main aim of surgery as it has been reported to improve the patient′s general status and enhance the efficacy of chemotherapy. [7] Griffiths and later other investigators have demonstrated that successful cytoreduction to a small-volume disease increases the chance of complete response and survival. [8],[9],[10],[11],[12] Bristow, in a meta-analysis of 6885 patients treated with platinum-based chemotherapy showed that every 10% increase in optimal surgery produces a 5.5% increase in median survival. [13] The goal of surgery thus is "optimal cytoreduction". However the term optimal cytoreduction has been a moving target and the volume of residual disease considered as optimal has consistently decreased over years, in various studies. The minimum size of residual disease associated with a significant impact on survival is exactly not known. However, in general best prognosis is ascribed to those patients who have no macroscopic disease left behind. [14],[15],[16] Traditionally, removal of uterus has been an integral part of surgery, irrespective of intent (viz. staging or debulking). As the chance of cure and long-term control of cancer has increased over the years because of better understanding of the biology of disease and improvement in treatment modalities, morbidity of treatment and the quality of life have become major issues in cancer treatment, which has led to the paradigm shift from radical resection to organ preservation. This has been a trend in malignancies at other sites, viz., breast, head and neck, etc., and has become a point of focus in ovarian malignancies also. Conservative surgery is a widely accepted option in germ cell tumors of ovary whether early or advanced, where preservation of uninvolved ovary and uterus is the standard of care. [17] Similarly several authors [18],[19],[20] have suggested that selected patients with early stage-invasive EOC can be managed successfully with fertility sparing surgery. Even when both the ovaries are removed the uninvolved uterus can still be conserved which gives at least a ray of hope to the woman or the couple, given the multiple options of artificial fertilization available today. But an obvious hindrance in doing the same is the possibility of extension of disease to uterus, given its anatomical proximity and vascular connections with the ovary. Since tumor residuum is the principal factor proved to affect the outcome in advanced ovarian cancer. This in itself proclaims that removal of structures other than tumor will not add to the survival. Since ovarian cancer spreads primarily by intraperitoneal route, uninvolved uterus can be equated to any other uninvolved abdominal organ preserved during cytoreduction. There are very few studies that have assessed uterine involvement in ovarian cancer. In an autopsy study of 100 women with diagnosed ovarian cancer, Dvoretsky et al. [21] evaluated the pattern of spread of ovarian carcinoma. Serous carcinoma was the most common histologic type (50%) noted and most of their patients had advanced disease at presentation (75%). Grade I tumor was present in only 6% of cases, whereas, grade II constituted over half of the cases (52%), and grade III (42%) the rest. Their cohort matches with ours in terms of histology (although we had higher proportion of serous tumors), stage and grade distribution. They evaluated all body sites for metastases and in addition all surgical pathologic material collected at the time of diagnosis and during the clinical course of the patient was reviewed. They reported a uterine serosal involvement in 27% and myometrial involvement in 10%. Cervical involvement was noted in 3% and interestingly vaginal involvement on autopsy was seen in 14%. We noted serosal involvement in only 15%, which is less than what is reported in their study but myometrial involvement was found in a similar proportion of patients as theirs. Myometrial involvement was in the form of local invasion from serosal surface and no cases of isolated myometrial metastases were noted. Thus the microscopic findings corroborated with the gross findings in our patients. Only one patient with grossly uninvolved uterus had an endometrial polyp with serous papillary cells on surface. Whether this was a synchronous primary or metastasis from ovary could not be ascertained. Raspagliesi et al. [18] reported their experience with 10 patients of invasive EOC and with high-grade or limited extraovarian disease treated with conservative surgery. Two patients were FIGO IIIA, four IIIC, whereas rest had early ovarian cancer. All patients were alive and disease-free at a median follow-up of 70 months (range 24-138 months). Nine patients were menstruating regularly and three had become pregnant. Colombo et al. [22] shared their experience of conservative surgery in 24 patients of ovarian cancer. Out of these one patient had stage II, one had IIIA and two had stage IIIC at presentation. They experienced recurrences in three patients, out of which one patient had stage II and one IIIC disease. One of these (IIIC) was salvaged with further surgery and chemotherapy. None of these patients had a uterine recurrence. In a review of 152 patients of EOC treated with conservative surgery, Colombo et al. [22] noted relapse in 18 patients, but none of them was reported to have uterine relapse. Thus these studies provide an indirect evidence for absence of microscopic uterine involvement, when it is grossly free, thus proving feasibility of uterine conservation even in selective cases with advanced disease. Presence of synchronous endometrial cancer is another concern in these patients. The occurrence of synchronous malignancy in ovary and endometrium is rare. Further it poses a diagnostic dilemma, as it could represent one of the following three situations: primary endometrial cancer with ovarian metastasis, primary ovarian cancer with endometrial metastasis, or synchronous primary endometrial and ovarian cancers. Pathologic criteria to distinguish synchronous primary cancers from metastatic lesions were proposed by Ulbright and Roth [23] first, and later revised by Scully et al. [24] Zaino et al. [25] have reported a relatively high incidence (10%) of co-existent endometrial carcinoma in ovarian cancer. Chiang et al. [26] reported a relatively low (2.7%) occurrence of synchronous endometrial carcinoma in these patients. In our study we noted only one (0.8%) case of co-existent endometrial carcinoma. Unlike western countries the incidence of endometrial cancer itself is very low in India, so the chance of having synchronous endometrial carcinoma is also likely going to be low. Should the possibility of simultaneous carcinoma of endometrium affect the treatment strategy, logically pre-operative diagnosis will not have much impact on routine management. However when uterine conservation is planned and/or patient gives history menstrual abnormalities an endometrial sampling/hysteroscopy is recommended. The absence of any correlation between uterine involvement and stage, histology, and laterality shows that uterus is not the preferred site for metastasis in EOC. The higher predilection for high-grade tumors to invade the uterus demonstrates their biological aggressiveness. But even then, the involvement is in the form of local invasion rather than metastasis. Conclusions In most cases of EOC, uterus is grossly free of tumor. The microscopic involvement of uterus can be excluded with confidence in cases without gross uterine involvement and low to intermediate grade tumors. Uterine involvement is independent, of stage of disease, histology and bilaterality or preoperative chemotherapy. There is a significantly high predilection for high-grade tumors to involve uterus. Incidence of synchronous endometrial cancer was very low in our study. Hence our data provides a good basis to evaluate the prospectus of uterine preservation in patients with EOC even in advanced cases without gross uterine involvement and having low-to-intermediate grade tumors. However the safety of this approach needs to be confirmed in adequately powered prospective trials. Acknowledgment Dr. Durga Vijayasree of Department of Gynaecological Oncology, Amrita Institute of Medical Sciences and Research Centre, Kochi, Kerala, India. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11128t3.jpg] [cn11128t5.jpg] [cn11128t6.jpg] [cn11128t2.jpg] [cn11128t4.jpg] [cn11128t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}