 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
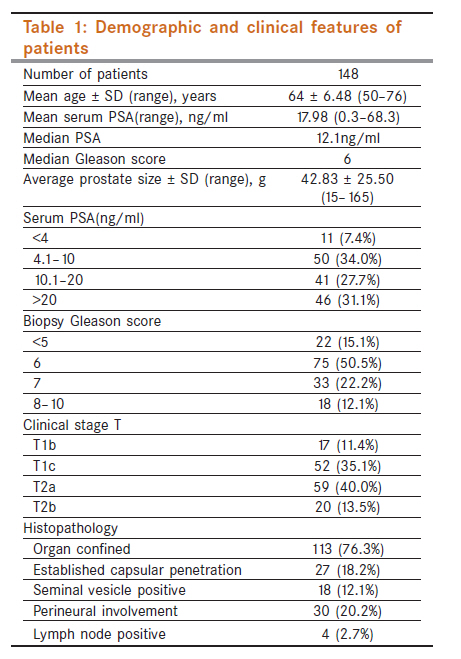
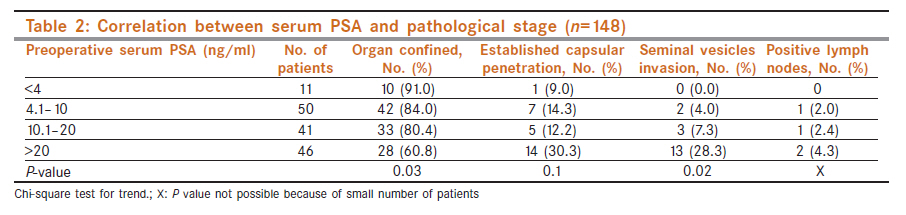
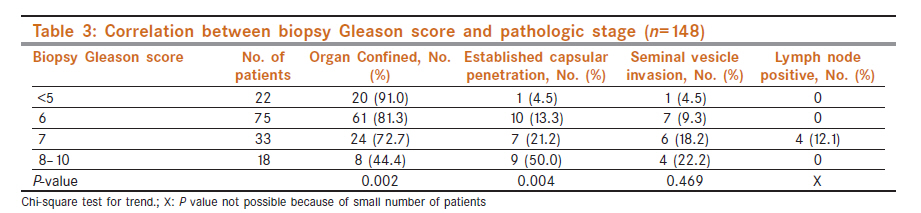
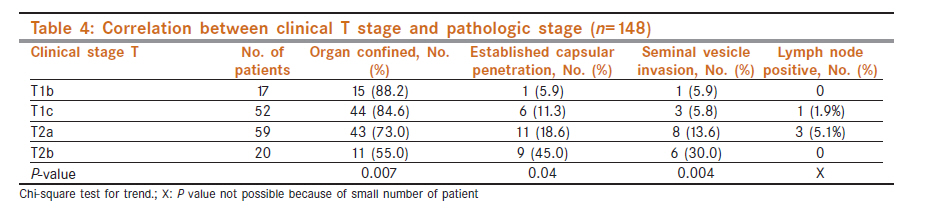
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 483-487 Genitourinary - Original Article Correlation between the preoperative serum prostate specific antigen, Gleason score, and clinical staging with pathological outcome following robot-assisted radical prostatectomy: An Indian experience P Singh1, PN Dogra1, NP Gupta2, R Nayyar1, A Seth1, TD Javali1, R Kumar1 1 Department of Urology, AIIMS, New Delhi, India Code Number: cn11130 PMID: 22293265 Abstract Objectives: To correlate the preoperative serum prostate specific antigen (PSA), Gleason score, and clinical staging with pathological outcome following robot-assisted radical prostatectomy (RARP) in Indian men with clinically localized cancer prostate. Keywords: Gleason score, prostate cancer, radical prostatectomy, staging Introduction Prostate cancer is one of the leading cancer types in urban India. It is now the third commonest male cancer in Delhi, fourth in Mumbai, fifth in Bangalore, and ninth in Chennai. [1],[2] Early detection may be behind this increasing trend in urban areas. Availability of prostate specific antigen (PSA) and prostate biopsy has resulted in increased diagnosis of prostate cancer, but many patients still present with locally advanced or metastatic stage in our country. In comparison to western population, [3] Indian patients usually have higher serum PSA and higher Gleason score on biopsy which may be because of late presentation. For an individual case, the oncological outcome depends not only on the surgical technique but also several factors such as PSA, Gleason score, and TNM stage. [4] Partin et al (1997) have earlier established probability tables combining parameters of serum PSA, Gleason score, and clinical stage in American population to predict prostate cancer extension. These tables were made based on large number of men who underwent radical prostatectomy with precise determination of pathologic stage. [5] But in Indian population, no such evaluation has yet been done, owing to the few number of cases that were offered radical prostatectomy due to various reasons. Increased number of radical prostatectomies following installation of the daVinci robotic system at our center has provided an opportunity to assess the pathological outcomes following radical prostatectomy in Indian scenario. Materials and Methods Hundred sixty-six men with clinically localized prostate cancer underwent robot -assisted radical prostatectomy (RARP) from June 2006 to October 2009 using daVinci S robotic system at our institute. We excluded 13 cases that received neoadjuvant hormonal treatment from the purview of this study, because it may have a bearing on final histopathological outcome. Other five patients who had final histopathology other than adenocarcinoma were also excluded. Preoperative assessment included detailed history and clinical examination along with serum PSA, biopsy Gleason score, bone scan, and contrast -enhanced computed tomography scan or magnetic resonance imaging in all cases. Clinical staging was done as per TNM staging, [6] and only cases with clinical T 1-2 , N 0 , M 0 were considered for RARP. All cases were done using the modified VIP technique of RARP. We ligated deep venous complex just before division of urethra, and only external iliac and obturator lymph nodes were removed. Lymphadenectomy was done in all cases as a part of study protocol. Fifty -three patients underwent unilateral nerve sparing and 28 patients underwent bilateral nerve-sparing radical prostatectomy. All preoperative biopsy slides and postoperative specimens were studied by trained uro-pathologists at our institute. Details of histopathological assessment were gathered including final Gleason score, capsular penetration, seminal vesicle, or lymph node involvement in all cases. Preoperative parameters were then analyzed in relation with postoperative histopathological findings using appropriate statistical methods including chi-square test for trend. A P-value less than 0.05 was considered statistically significant. Fifteen patients were diagnosed on less than six cores, 59 on six core transrectal ultrasound-guided prostate biopsy. Eighteen patients were diagnosed post-TURP; 7-12 core biopsies were done in the remaining 56 patients. Results Data were analyzed for 148 patients constituting the study group. The mean (range) age of patients was 64 ± 6.48 (50-76) years and mean (range) body mass index was 25.29 ± 3.72 (16-34) kg/m 2 . The mean (range), median preoperative serum PSA, and median Gleason score in these patients were 17.98 (0.3-68.3) ng/ml, 12.1 ng/ml, and 6, respectively. There was palpable tumor (T2a, T2b) in 79 patients, and in 69 patients tumor was nonpalpable (T1b,T1c) being detected on PSA screening or TURP. Detailed preoperative profile of the cases is given in [Table - 1]. When only primary grade was considered, 47 patients (32%) showed increase in grade and 16 patients (11%) had decrease in grade on specimen histopathology when compared with preoperative Gleason score. On considering secondary grade, increase in grade was seen in 40 patients (27%) and decrease in grade in 7 patients (5%). Average Gleason score of specimen histopathology was 6.10 ± 1.5. Organ-confined disease was reported in 113 (76.3%) patients. Extracapsular peneteration was seen in 27 (18.2%) patients. In all, 18 (12.1%) patients had seminal vesicle involvement in final histopathology report. Nine cases had both seminal vesicle and capsular involvement. Perineural involvement was found in 30 (20.2%) patients. Lymph node metastasis was found in 4 (2.7%) patients. Average number of lymph nodes isolated on the histopathology specimen was 3.6. Correlation of preoperative serum PSA with histopathological outcomes The details of histopathological outcomes in various PSA subgroups are given in [Table - 2]. On correlating serum PSA with final pathology, it was found that with increasing serum PSA, the organ confinement of disease decreases linearly, reaching upto 60% in patients with PSA more than 20 ng/ml (P=0.03). Seminal vesicle involvement also increases linearly in a significant manner (P=0.02) with increase in serum PSA levels. Similarly, capsular penetration and lymph node involvement increase with increase in serum PSA levels but not in linear or significant manner. Importantly, there were nine cases in the group with PSA more than 20 ng/ml that had both seminal vesicle involvement and capsular penetration suggesting poorer histopathological and possibly poorer long-term oncological outcome for this group. Correlation of biopsy Gleason score with histopathological outcomes On correlating preoperative Gleason score with pathological outcome [Table - 3], it was found that with increase in preoperative biopsy Gleason score, organ confinement of cancer decreases linearly and significantly (P=0.002). Capsular penetration also increases with increase in biopsy Gleason score and is maximum in patients with Gleason score 8 or more (P=0.004). But seminal vesicle involvement did not correlate with increase in Gleason score. Correlation of clinical T stage with histopathological outcomes Correlation of clinical T stage with pathological outcome [Table - 4] shows that organ confinement of disease decreases progressively with increase in clinical stage. This relationship was linear and clinically significant (P=0.007). Similarly, capsular penetration (P=0.04) and seminal vesicle (P=0.004) involvement increased significantly with increase in clinical stage. Discussion Studies have found that clinical examination alone cannot predict the pathological outcome and is therefore not the ideal method to decide the mode of treatment. [7],[8],[9],[10],[11] Several preoperative parameters have been assessed to predict the actual pathologic stage and outcome after treatment. Pre- and postoperative nomograms have been devised to identify patients in which a high risk of extraprostatic disease [12] or disease progression is expected. [13],[14] Presently, preoperative serum PSA, Gleason score from biopsy, and clinical stage are the most common parameters used to predict the pathological outcome, prognosticate, or choose a definitive treatment in patients with prostate cancer [15] However, there is no available reference data of pathological outcomes in Indian population for radical prostatectomy. The finding of an organ-confined disease after radical retropubic prostatectomy varies from 13% to 82% of cases. [15],[16] In 1993, Partin et al prepared nomograms using PSA, clinical stage, and biopsy Gleason score to predict prostate cancer extension. [15] .The percentage of organ-confined disease following radical prostatectomy at John Hopkins Hospital between 1987 and 1982 (prior to introduction of nomograms) was 33%. Since the use of Partin nomograms (1993-1996), 55% had organ-confined disease representing a 20% improvement over the "pre-nomogram". [17] According to Partin et al,[17] PSA screening led to stage migration which may be the cause of this improvement, but no staging modality was introduced in this time frame except for these nomograms. That can explain this major shift in pathological findings. Crippa et al[18] found organ-confined disease in 66.7% of cases. In our study, we found overall 76.3% had organ-confined disease. We also found a direct linear correlation of pathological outcome with biopsy Gleason score, serum PSA levels, and clinical stage. Crippa et al[18] made a nomogram which did not include clinical stage (as proposed by Partin et al) because they believed this variable was not clinical significant. Several other models using different variables have also been developed to predict disease extension and/or recurrence. [19],[20],[21],[22],[23] But some of them are not clinically practicable due to the complexity of interpretation. In a review of 703 patients of radical retropubic prostatectomy for clinically localized prostate cancer, Partin et al found that 75% of men with PSA less than 4.0 ng/ml, 53% with PSA between 4.0 and 10 ng/ml, and 26% with PSA between 10 and 20 ng/ml had organ-confined disease. [15] In our study, these rates were 91.0%, 84.0%, and 80.4%, respectively. Our results of higher percentage of cases having localized disease are consistent with the fact that higher PSA values seen in Asian/Indian men may be due to a component of BPH or chronic prostatitis or diagnosis not based on PSA screening. This also highlights the need of developing nomograms as per Indian standards. We have shown correlation of capsular penetration and seminal vesicle involvement with increasing PSA, Gleason grade, or clinical T stage in Indian patients, although change in capsular penetration rate with change in PSA did not reach level of clinical significance in this study. The limitations of this study were small sample size of the study population, small number of patients who had seminal vesicle invasion and lymph node metastasis. Lymph node yield was also less which could have led to understaging of the disease. Another limitation is that we have not calculated the tumor volume in histopathology specimen. There was a selection bias in this study as all the patients are clinical stage T1 or T2 tumors. We did computed tomography / magnetic resonance imaging staging staging of tumor preoperatively in every patient. In spite of that 27 patients had capsular penetration, 18 had seminal vesicle invasion and 4 patients had lymph node metastasis. This also stated the understaging of tumor clinically and radiolologically. Few cases had multiple overlapping histopathological findings, including one patient in T1c group with seminal vesicle involvement, capsular penetration, and lymph node metastasis; three patients in T2a group with both capsular and lymph node involvement; and six patients in T2b group with both seminal vesicle and capsular involvement. The increasing frequency of multiple histopathological poor outcome parameters in one patient again emphasizes this trend of poorer outcome with increasing clinical stage. Based on these results and with the increasing number of cases along with some help from our pathology colleagues to review the whole mount specimen, we shall be able to develop a nomogram to predict likelihood of extraprostatic disease before the surgery in Indian population. The primary value of nomograms is to council the patients preoperatively regarding the probability of their tumor specific pathological stage following surgery. Nonetheless, this study provides a forward footstep toward gathering some bankable Indian data to rely upon for building future larger studies in this regard. Conclusions Pathological outcome after radical prostatectomy has a clinically significant indirect correlation with the preoperative serum PSA, biopsy Gleason score, and clinical stage. Compared with western literature, the chances of organ confined disease are somewhat higher in Indian men for same level of PSA. Combination of above parameters can be used to develop nomograms and predict the pathological outcome following radical prostatectomy in Indian population in future. It is also important to council the patient before surgery of the ultimate outcome following surgery. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11130t1.jpg] [cn11130t4.jpg] [cn11130t3.jpg] [cn11130t2.jpg] |
| |||||||||


{kind=link}
{kind=link}
{kind=link}
{kind=link}