 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
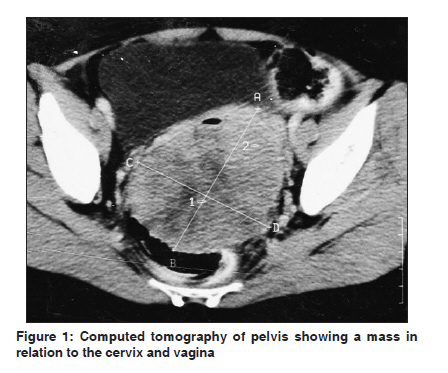
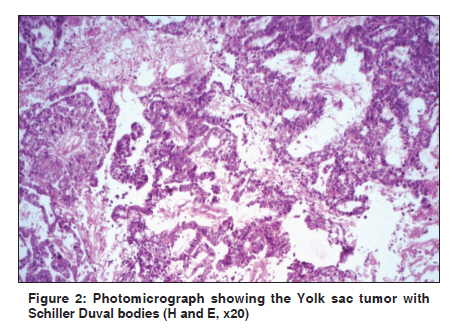
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 515-516 Letter to Editor Primary yolk sac tumor of cervix and vagina in an adult female: A rare case report K Mardi, N Gupta, R Bindra Department of Pathology, Indira Gandhi Medical College, Shimla, Himachal Pradesh, India Code Number: cn11137 PMID: 22293272 Sir, Most Endodermal Sinus Tumors (EST) occur in the ovaries and testes of young patients and are usually related to midline structures. The vagina is an extremely rare site for primary germ cell tumors. [1] We present a rare case of extragonadal yolk sac tumor arising in the cervicovaginal region of a 27-year-old female. A 20-year-old female presented with difficulty in passing stools and pain in the perianal region since one month. In addition she also complained of bleeding per vagina. On pervaginal examination a hard mass was felt in the posterior wall and lateral fornices of the vagina. On per rectal examination, a large endocervical mass was felt and the rectal mucosa was free. The case was clinically diagnosed as carcinoma cervix. A computed tomography (CT) scan revealed a hypodense to isodense retrovesical mass, 4 x 4 cm in size, in relation to the cervix, revealing heterogeneous intense enhancement, after IV contrast [Figure - 1]. The patient underwent laparotomy. Preoperatively, a large globular soft tissue mass arose from the cervix and involved the upper one-third of the vagina. Now it was clinically diagnosed as a cervical fibroid. The tumor was excised and we received multiple gray white soft tissue masses, together measuring 8 cm 3 . The cut surface of these soft tissue masses were gray white with yellowish areas and minute cystic areas filled with mucin. On microscopic examination, the tumor showed more than one histopathological pattern. Three major patterns were found: festoon, reticular, and solid. The festoon pattern showed anastomosing channels and tubules lined with cuboidal epithelial cells, with vacuolated cytoplasm and hyperchromic nuclei, associated with the formation of Schiller-Duval bodies [Figure - 2]. A reticular pattern consisting of a loose network of cystic spaces lined by flattened epithelial cells was also present. Occasional intracellular and extracellular hyaline bodies were present. These hyaline bodies were PAS-positive and resistant to diastase digestion. With these characteristic histological findings the tumor was diagnosed as a Yolk sac tumor (YST) of the cervix and vagina. The serum alpha feto protein levels measured during the immediate postoperative period were also high (1210 ng/ml), thus supporting our diagnosis. The YST of the cervix and vagina is extremely rare, a highly malignant germ cell tumor that exclusively involves children less than three years of age. [2],[3] Allyn et al, [4] have described two such cases in women over 20 years of age. However, both these cases were questionable. One had unconvincing histological evidence and the other represented an advanced ovarian germ cell neoplasm. A clearly defined YST of the vagina and cervix in an adult female is exceptional. Among the 50 reported cases of EST in world literature, 10 - 15% originate in the cervix and 50% in the vagina, whereas, the vulva and corpus are extremely rare sites.[1] The clinical presentation includes a history of bloody vaginal discharge, often accompanied by a polypoid mass protruding from the vagina. Pervaginal examination, best performed under anesthesia, demonstrates a lesion that is polypoid and friable arising from the vagina or cervix. With this clinical presentation it is not surprising that many are clinically misdiagnosed as sarcoma botryoides (embryonal rhabdomyosarcoma). The histogenesis of this rare tumor is uncertain. As in the case of other primary extragonadal germ cell tumors, the aberrant migration of germ cells during early embryonic life, from the yolk sac to the gonadal ridges, remains a distinct possibility. [5] The origin is also thought to be the embryonic remnants of midline mesonephric structures. [6] Endodermal Sinus Tumors are locally aggressive and capable of metastasis via the hematogenous as well as lymphatic routes. Simple tumor excision is not sufficient, as residual cells induce recurrence and make chemotherapy ineffective. The serum alpha-fetoprotein (AFP) level is a useful marker for the diagnosis and monitoring of the recurrence of vaginal EST. Abdominal total hysterectomy with bilateral salpingo-oophorectomy has been the standard treatment so far. However, recently adjuvant chemotherapy with a combination of multiple chemotherapeutic agents has been added to improve the survival rate in these patients. To conclude, EST, although rare, requires a proper diagnosis. This tumor must be differentiated from clear cell adenocarcinoma, which is more aggressive and less chemosensitive. Diastase-resistant and PAS-positive hyaline intracytoplasmic globules are diagnostic, with high levels of AFP. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11137f2.jpg] [cn11137f1.jpg] |
| |||||||||

{kind=link}
{kind=link}