 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
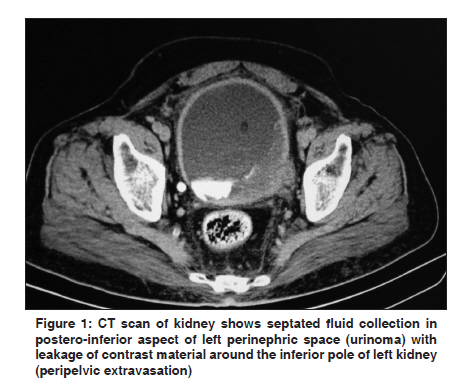
Indian Journal of Cancer, Vol. 48, No. 4, October-December, 2011, pp. 516-517 Letter to Editor A case report: Urinoma as initial presenting sign of bladder malignancy SAA Rizvi1, A Ibne2, MA Siddiqui2, MDQ Syed2 1 Department of Surgery, Jawaharlal Nehru Medical College, Aligarh Muslim University, Aligarh, India Code Number: cn11138 PMID: 22293273 Sir, Urinoma is an encapsulated collection of extravasated urine which is most commonly caused by renal trauma. Urinoma formation as first manifestation of urinary bladder carcinoma is uncommon. We report a case of bladder carcinoma in an elderly man who first presented in emergency department with urinoma formation. A 65-year-old man was doing well until the day of admission, when he became drowsy and disoriented. Past history was positive for mild back pain. On per-abdomen examination, a ballotable mass was noticed in the left lumbar region. Urinalysis revealed hematuria and proteinuria. Blood biochemistry revealed normal renal function except for electrolyte imbalance (serum sodium: 125 mmol/l; serum potassium: 3.0 mmol/l; serum chloride: 100 mmol/l). Abdominal ultrasonography demonstrated mild hydrouretronephrosis on the left side with a septated cystic collection in perinephric space. The urinary bladder was empty at the time of examination. The computed tomographic (CT) scan confirmed the presence of left side urinoma with leakage of contrast material around the inferior pole of left kidney suggestive of peripelvic extravasation [Figure - 1]. Further scanning of pelvis demonstrated a hyperdense bladder mass involving left postero-lateral wall and vesicouretric junction with urinary tract obstruction leading to urinoma formation [Figure - 2]. A cystoscopic-guided biopsy of the lesion showed well-differentiated muscle invasive tumor. Ultrasound-guided percutaneous drainage of the left perirenal collection was done. The contents of the fluid were similar to urine, thus providing strong evidence that the collection was urinoma. The patient was categorized according to TNM as T2 (muscle invasive), N0 (no regional lymph node metastasis), and M0 (no distant metastasis) and radical cystectomy was done. Final histopathology examination confirmed the lesion to be muscle invasive (T2). Urinary diversion was done in a continent pouch created from an ileal segment. Urinoma is caused by extravasation of urine. [1] Three essential factors are required for formation of urinoma: a functioning renal unit, breach in the pelvicalyceal system, and ureteral obstruction. [2] Urine causes lipolysis and inflammation of perirenal fat with formation of a fibrous capsule around the collected urine. Urinoma occurs most commonly following renal trauma. [3] Other common causes are ureteral tumor and calculus in adults, and posterior urethral valves and ureteropelvic junction obstruction in children. Abdominal ultrasound is the initial screening procedure. However, CT is better in demonstrating relationship of the urinoma with surrounding structures. [4] Urinoma is usually unopacified on initial early scans but fill in the delayed scans, thereby documenting continuity between the collecting system and the urinoma. [4] Aspiration of the cystic collection under ultrasound or CT guidance is both diagnostic and therapeutic. The treatment of urinoma requires prompt diagnosis with delineation of the cause else it could lead to complications like urinary peritonitis, parapelvic urine granuloma, periureteral fibrosis, abscess formation, and sepsis. Once the underlying obstruction is rectified, most urinoma′s resolve spontaneously. In urinoma resulting from carcinoma of the urinary bladder where immediate treatment in emergency department is not desired, drainage is a reasonable first step before surgical correction. Among drainage modalities, percutaneous drainage is the recommended procedure when the patient is hemodynamically stable and the urinoma is fixed. [5] We emphasize that all urinomas should be thoroughly evaluated by radiologic imaging for an underlying cause. Immediate drainage under ultrasound or CT guidance is a reasonable first-step treatment before surgical correction is done as any delay can lead to serious complications. References
Copyright 2011 - Indian Journal of Cancer The following images related to this document are available:Photo images[cn11138f1.jpg] [cn11138f2.jpg] |
| |||||||||

{kind=link}
{kind=link}